J Korean Med Sci.
2009 Aug;24(4):668-673. 10.3346/jkms.2009.24.4.668.
A Prospective Study on the Incidence and Predictive Factors of Relative Adrenal Insufficiency in Korean Critically-Ill Patients
- Affiliations
-
- 1Divisions of Pulmonary and Critical Care Medicine, Department of Medicine, Samsung Medical Center, Sungkyunkwan University School of Medicine, Seoul, Korea. suhgy@skku.edu
- 2Division of Endocrinology, Department of Medicine, Samsung Medical Center, Sungkyunkwan University School of Medicine, Seoul, Korea.
- KMID: 1779201
- DOI: http://doi.org/10.3346/jkms.2009.24.4.668
Abstract
- This study was undertaken to evaluate the incidence and risk factors associated with relative adrenal insufficiency (RAI) in Korean critically-ill patients. All patients who were admitted to the Medical Intensive Care Unit (MICU) of Samsung Medical Center between January 1, 2006 and April 30, 2007 were prospectively evaluated using a short corticotropin stimulation test on the day of admission. RAI was defined as an increase in the serum cortisol level of <9 microgram/dL from the baseline after administration of 250 microg of corticotropin. In all, 123 patients were recruited and overall the incidence of RAI was 44% (54/123). The presence of septic shock (P=0.001), the Simplified Acute Physiology Score (SAPS) II (P=0.003), the Sequential Organ Failure Assessment (SOFA) score (P=0.001), the mean heart rate (P=0.040), lactate levels (P=0.001), arterial pH (P=0.047), treatment with vasopressors at ICU admission (P=0.004), and the 28-day mortality (P=0.041) were significantly different between patients with and without RAI. The multivariate analysis showed that the SOFA score was an independent predictor of RAI in critically-ill patients (odd ratio=1.235, P=0.032). Our data suggest that RAI is frequently found in Korean critically-ill patients and that a high SOFA score is an independent predictor of RAI in these patients.
Keyword
MeSH Terms
-
Adrenal Insufficiency/diagnosis/*epidemiology/mortality
Adrenocorticotropic Hormone/diagnostic use
Adult
Aged
*Critical Illness
Female
Humans
Hydrocortisone/blood
Intensive Care Units
Korea
Male
Middle Aged
Multivariate Analysis
Predictive Value of Tests
Prospective Studies
ROC Curve
Risk Factors
Severity of Illness Index
Survival Rate
Figure
-
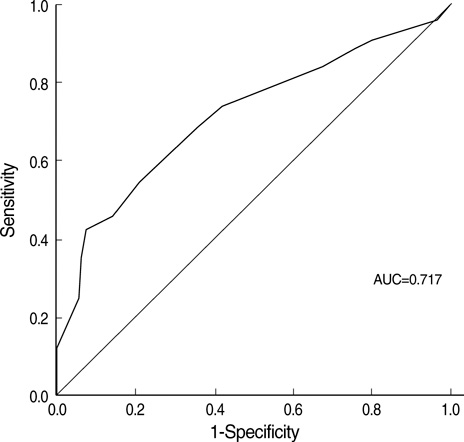
Fig. 1 Receiver operator curve (ROC) analysis of Sepsis-Related Organ Failure scores predicting adrenal insufficiency in critically-ill patients. AUC, area under the ROC curve.
Cited by 1 articles
-
Prognostic Implication of Adrenocortical Response during the Course of Critical Illness
Jin Hwa Song, Jung Hee Kim, Sang-Min Lee, Jinwoo Lee
Acute Crit Care. 2019;34(1):38-45. doi: 10.4266/acc.2018.00339.
Reference
-
1. Schein RM, Sprung CL, Marcial E, Napolitano L, Chernow B. Plasma cortisol levels in patients with septic shock. Crit Care Med. 1990. 18:259–263.
Article2. Drucker D, McLaughlin J. Adrenocortical dysfunction in acute medical illness. Crit Care Med. 1986. 14:789–791.
Article3. Drucker D, Shandling M. Variable adrenocortical function in acute medical illness. Crit Care Med. 1985. 13:477–479.
Article4. Annane D, Sebille V, Troche G, Raphael JC, Gajdos P, Bellissant E. A 3-level prognostic classification in septic shock based on cortisol levels and cortisol response to corticotropin. JAMA. 2000. 283:1038–1045.
Article5. Marik PE. Mechanisms and clinical consequences of critical illness associated adrenal insufficiency. Curr Opin Crit Care. 2007. 13:363–369.
Article6. Dimopoulou I, Tsagarakis S, Kouyialis AT, Roussou P, Assithianakis G, Christoforaki M, Ilias I, Sakas DE, Thalassinos N, Roussos C. Hypothalamic-pituitary-adrenal axis dysfunction in critically ill patients with traumatic brain injury: incidence, pathophysiology, and relationship to vasopressor dependence and peripheral interleukin-6 levels. Crit Care Med. 2004. 32:404–408.
Article7. Kilger E, Weis F, Briegel J, Frey L, Goetz AE, Reuter D, Nagy A, Schuetz A, Lamm P, Knoll A, Peter K. Stress doses of hydrocortisone reduce severe systemic inflammatory response syndrome and improve early outcome in a risk group of patients after cardiac surgery. Crit Care Med. 2003. 31:1068–1074.
Article8. Marik PE, Kiminyo K, Zaloga GP. Adrenal insufficiency in critically ill patients with human immunodeficiency virus. Crit Care Med. 2002. 30:1267–1273.
Article9. Sheridan RL, Ryan CM, Tompkins RG. Acute adrenal insufficiency in the burn intensive care unit. Burns. 1993. 19:63–66.
Article10. Sibbald WJ, Short A, Cohen MP, Wilson RF. Variations in adrenocortical responsiveness during severe bacterial infections. Unrecognized adrenocortical insufficiency in severe bacterial infections. Ann Surg. 1977. 186:29–33.11. Hamrahian AH, Oseni TS, Arafah BM. Measurements of serum free cortisol in critically ill patients. N Engl J Med. 2004. 350:1629–1638.
Article12. Annane D, Bellissant E, Sebille V, Lesieur O, Mathieu B, Raphael JC, Gajdos P. Impaired pressor sensitivity to noradrenaline in septic shock patients with and without impaired adrenal function reserve. Br J Clin Pharmacol. 1998. 46:589–597.
Article13. Hoen S, Asehnoune K, Brailly-Tabard S, Mazoit JX, Benhamou D, Moine P, Edouard AR. Cortisol response to corticotropin stimulation in trauma patients: influence of hemorrhagic shock. Anesthesiology. 2002. 97:807–813.14. Grinspoon SK, Biller BM. Clinical review 62: laboratory assessment of adrenal insufficiency. J Clin Endocrinol Metab. 1994. 79:923–931.
Article15. Beishuizen A, Thijs LG. Relative adrenal failure in intensive care: an identifiable problem requiring treatment? Best Pract Res Clin Endocrinol Metab. 2001. 15:513–531.
Article16. Annane D, Sebille V, Charpentier C, Bollaert PE, Francois B, Korach JM, Capellier G, Cohen Y, Azoulay E, Troche G, Chaumet-Riffaut P, Bellissant E. Effect of treatment with low doses of hydrocortisone and fludrocortisone on mortality in patients with septic shock. JAMA. 2002. 288:862–871.
Article17. Sprung CL, Annane D, Keh D, Moreno R, Singer M, Freivogel K, Weiss YG, Benbenishty J, Kalenka A, Forst H, Laterre PF, Reinhart K, Cuthbertson BH, Payen D, Briegel J. Hydrocortisone therapy for patients with septic shock. N Engl J Med. 2008. 358:111–124.
Article18. Annane D, Maxime V, Ibrahim F, Alvarez JC, Abe E, Boudou P. Diagnosis of adrenal insufficiency in severe sepsis and septic shock. Am J Resp Crit Care Med. 2006. 174:1319–1326.
Article19. Meikle AW, Jubiz W, Matsukura S, West CD, Tyler FH. Effect of diphenylhydantoin on the metabolism of metyrapone and release of ACTH in man. J Clin Endocrinol Metab. 1969. 29:1553–1558.
Article20. Kwon YS, Suh GY, Kang EH, Koh WJ, Chung MP, Kim H, Kwon OJ. Basal serum cortisol levels are not predictive of response to corticotropin but have prognostic significance in patients with septic shock. J Korean Med Sci. 2007. 22:470–475.
Article21. Yang Y, Liu L, Zhao B, Li MQ, Wu B, Yan Z, Gu Q, Sun H, Qiu HB. Relationship between adrenal function and prognosis in patients with severe sepsis. Chin Med J (Engl). 2007. 120:1578–1582.
Article22. Burke CW. Adrenocortical insufficiency. Clin Endocrinol Metab. 1985. 14:947–976.
Article23. Oelkers W. Adrenal insufficiency. N Engl J Med. 1996. 335:1206–1212.
Article24. Cooper MS, Stewart PM. Corticosteroid insufficiency in acutely ill patients. N Engl J Med. 2003. 348:727–734.
Article25. de Jong MF, Beishuizen A, Spijkstra JJ, Girbes AR, van Schijndel RJ, Twisk JW, Groeneveld AB. Predicting a low cortisol response to adrenocorticotrophic hormone in the critically ill: a retrospective cohort study. Crit Care. 2007. 11:R61.
Article
- Full Text Links
-
- Actions
-
Cited
- CITED
-
- Close
- Share
-
- Similar articles
-
- Relative Adrenal Insufficiency in Postresuscitation Patients
- Corticosteroid Treatment in Critically Ill Patients
- Polyuria and Natriuresis of Unknown Origin Accompanied with Hypotension in Critically Ill Patients
- Opioids Use and Adrenal Insufficiency
- Adrenal Insufficiency in Patients with Rotator Cuff Tear: Prevalence, Risk Factors and Influence on Outcome
