Ocular Motility Disturbances in Orbital Wall Fracture Patients
- Affiliations
-
- 1Department of Ophthalmology, Pochun CHA University College of Medicine, Pundang CHA Hospital, Sungnam, Korea. eye@cha.ac.kr
- KMID: 1734070
- DOI: http://doi.org/10.3349/ymj.2005.46.3.359
Abstract
- It is difficult to identify the exact cause of ocular motility disturbances in orbital wall fracture patients. By performing CT and ocular motility tests before and after surgery, this study analyzes the functions of the extraocular muscles and determines correlations between the results. Between February 2001 and January 2003, 45 eyes of 45 patients with orbital wall fractures, whose medical records could be traced back at least 6 months, underwent surgical repair in our hospital. All variables were analyzed using the independent t-test, paired t-test, and Chi-square test. There was no significant difference in the location and degree of fracture and the incarceration pattern of 6 patients who had moderate or severe diplopia, and of the remaining patients 6 months after surgery. However, in the case of diplopia, the sum of ocular motility limitation was 5.67 +/- 4.18, and the degree of extraocular motility disturbance was 3.67 +/- 2.42 before surgery. When there was no diplopia, the sum of ocular motility limitation was 1.13 +/- 1.38, and the degree of extraocular motility disturbance was 1.08 +/- 1.16 (p < 0.005, independent t-test). Ocular movement was successfully recovered by surgical reduction within 3 weeks from trauma. Postoperative ocular motility disturbance was more related to various ocular motility test results than CT findings. Ocular motility disturbances can remain after surgery if ocular motility limitation and extraocular motility disturbance are significant after trauma. Additional studies on the various tests to examine functions of extraocular muscles are required to identify and analyze the exact cause of ocular motility disturbance.
MeSH Terms
Figure
-
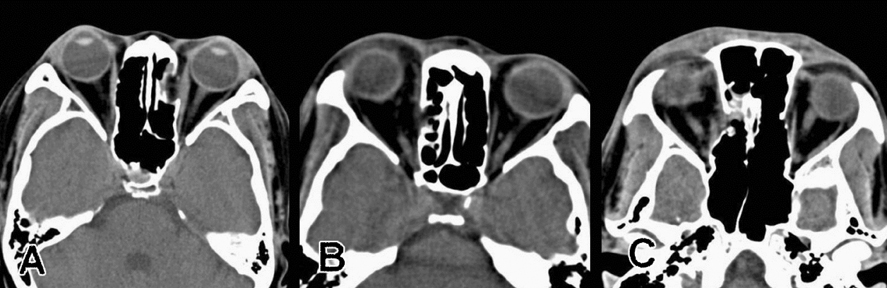
Fig. 1 Location of orbital fracture at medial wall. A: left anterior medial orbital wall, B: right middle medial wall, C: right posterior medial wall.
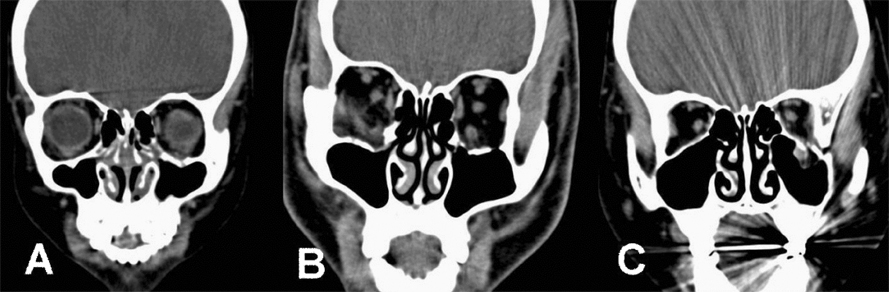
Fig. 2 Location of orbital fracture at inferior wall. A: left anterior inferior orbital wall, B: right middle inferior wall, C: left posterior inferior wall.
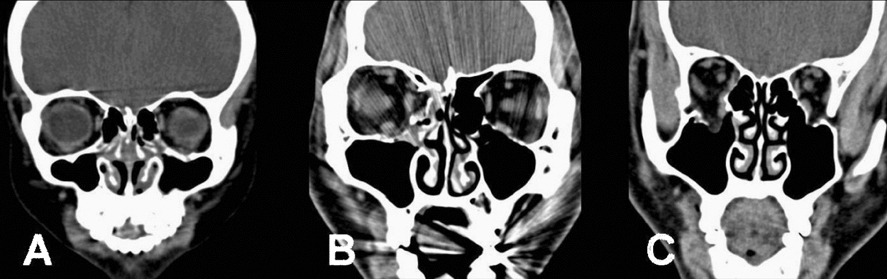
Fig. 3 Degree of orbital fracture according to the degree of orbital volume expansion and soft tissue prolapse. A: mild; minimal orbital expansion and soft tissue herniation, B: moderate; moderate expansion and prolapse, C: severe; significant expansion and prolapse.
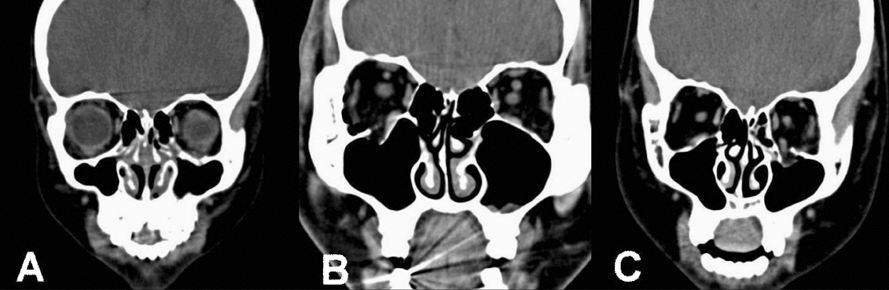
Fig. 4 Incarceration patterns of extraocular muscles in the orbital fracture. A: free; not continuous with any bony density in any of the scan, B: hooked; continuous with bone along one side, but majority of the muscle continuous only with soft tissue or fat densities, C: entrapped; adjacent to bone, nasally and temporally.
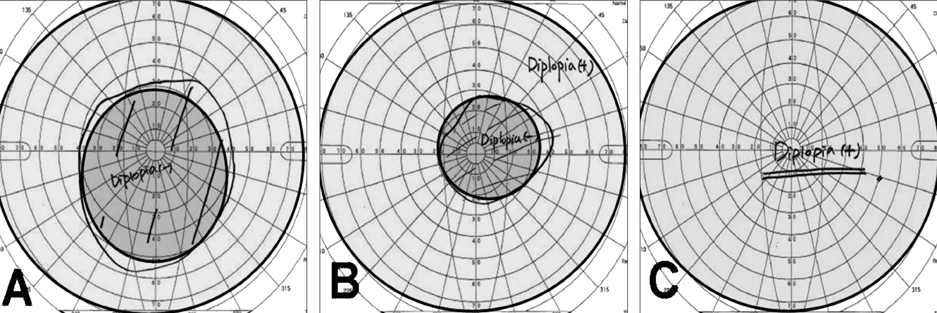
Fig. 5 The degree of diplopia was quantified by measuring the field of single binocular vision (blue shaded area). A: mild; diplopia appears more than 30 degrees from the primary position, B: moderate; diplopia appears more than 30 degrees between 10 and 30 degrees from the primary position, and C: severe; diplopia appears within 10 degrees from the primary position.
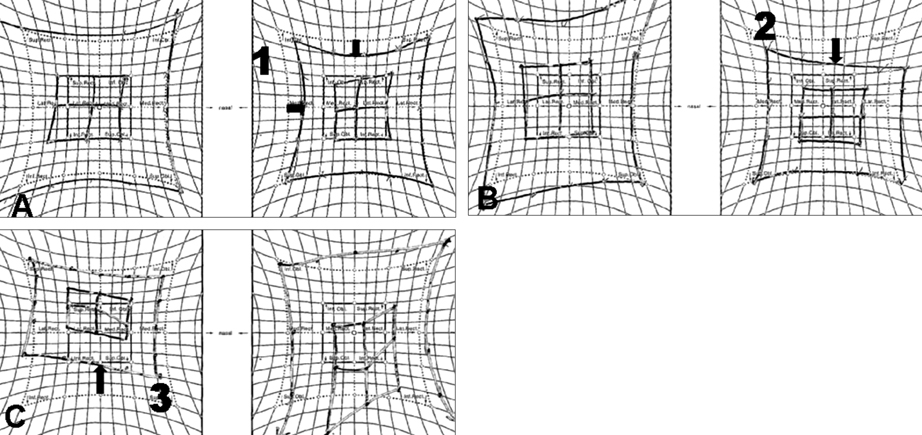
Fig. 6 The degree of extraocular motility disturbance was graded in 4 cardinal directions by the Hess screen test, 0 to 3 and added, where 0 indicates normal. A: mild; 1 degree reduction (arrow) of extraocular muscle power, B: moderate; 2 degree reduction (arrow), and C: 3 degree reduction (arrow) compared with the normal Hess screen test result.
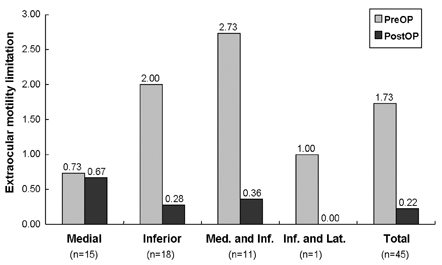
Fig. 7 The extraocular motility limitation according to the location of orbital wall fracture. The scores of ocular motility limitation (0-3) in each four directions were added up in each patient. (p < 0.005, paired t-test)

Fig. 8 The extraocular motility disturbance according to the location of orbital wall fracture. The scores of ocular motility disturbance (0-3) in each four directions were added for each patient. (p < 0.005, paired t-test)
Cited by 1 articles
-
The Size of Extraocular Muscles Estimated by Computed Tomography in Patients Undergoing Orbital Wall Fracture Repair
Hyoung Eun Kim, Helen Lew, Young Soo Yun
J Korean Ophthalmol Soc. 2009;50(10):1447-1454. doi: 10.3341/jkos.2009.50.10.1447.
Reference
-
1. Smith B, Regan WF Jr. Blow-out fracture of the orbit; mechanism and correction of internal orbital fracture. Am J Ophthalmol. 1957. 44:733–739.2. Bains RA, Rubin PA. Blunt orbital trauma. Int Ophthalmol Clin. 1995. 35:37–46.3. Wilkins RB, Havins WE. Current treatment of blow-out fractures. Ophthalmology. 1982. 89:464–466.4. Dortzbach RK, Elner VM. Which orbital floor blowout fractures need surgery? Adv Ophthalmic Plast Reconstr Surg. 1987. 6:287–289.5. Nathanson A, Matthis SP, Tengvar M. Diagnosis and treatment of fractures of the orbital floor. A ten-year retrospective study. Acta Otolaryngol Suppl. 1992. 492:28–32.6. Hawes MJ, Dortzbach RK. Surgery on orbital floor fractures. Influence of time of repair and fracture size. Ophthalmology. 1983. 90:1066–1070.7. Putterman AM, Stevens T, Urist MJ. Nonsurgical management of blow-out fractures of the orbital floor. Am J Ophthalmol. 1974. 77:232–239.8. Gilbard SM. Management of orbital blowout fractures: the prognostic significance of computed tomography. Adv Ophthalmic Plast Reconstr Surg. 1987. 6:269–280.9. Kulwin DR, Leadbetter MG. Orbital rim trauma causing a blowout fracture. Plast Reconstr Surg. 1984. 73:969–971.10. Waterhouse N, Lyne J, Urdang M, Garey L. An investigation into the mechanism of orbital blowout fractures. Br J Plast Surg. 1999. 52:607–612.11. Warwar RE, Bullock JD, Ballal DR, Ballal RD. Mechanisms of orbital floor fractures: a clinical, experimental, and theoretical study. Ophthal Plast Reconstr Surg. 2000. 16:188–200.12. Gilbard SM, Mafee MF, Lagouros PA, Langer BG. Orbital blowout fractures. The prognostic significance of computed tomography. Ophthalmology. 1985. 92:1523–1528.13. Gilbard SM. Management of orbital blowout fractures: the prognostic significance of computed tomography. Adv Ophthalmic Plast Reconstr Surg. 1987. 6:269–280.14. Okinaka Y, Hara J, Takahashi M. Orbital blowout fracture with persistent motility deficit due to fibrosis of the inferior rectus muscle and perimuscular tissue. Ann Otol Rhinol Laryngol. 1999. 108:1174–1176.15. Biesman BS, Hornblass A, Lisman R, Kazlas M. Diplopia after surgical repair of orbital floor fractures. Ophthal Plast Reconstr Surg. 1996. 12:9–16.16. Liu D. Blindness after blow-out fracture repair. Ophthal Plast Reconstr Surg. 1994. 10:206–210.17. Girotto JA, Gamble WB, Robertson B. Blindness after reduction of facial fractures. Plast Reconstr Surg. 1998. 102:1821–1834.18. Folkestad L, Westin T. Long-term sequelae after surgery for orbital floor fractures. Otolaryngol Head Neck Surg. 1999. 120:914–921.19. Jordan DR, St Onge P, Anderson RL. Complications associated with alloplastic implants used in orbital fracture repair. Ophthalmology. 1992. 99:1600–1608.20. Harley RD. Surgical management of persistent diplopia in blowout fractures of the orbit. Ann Ophthalmol. 1975. 7:1621–1626.21. Lisman RD, Smith BC, Rodgers R. Volkmann's ischemic contractures and blowout fractures. Adv Ophthalmic Plast Reconstr Surg. 1987. 7:117–131.22. Converse JM, Smith B, Obear MF, Wood-Smith D. Orbital blow-out fractures: a ten-year survey. Plast Reconstr Surg. 1967. 39:20–36.23. Greenwald HS Jr, Keeney AH, Shannon GM. A review of 128 patients with orbital fractures. Am J Ophthalmol. 1974. 78:655–664.24. Kim YI, Won IG. The Clinical Findings in 24 cases of orbital blow-out fracture. J Korean Ophthalmol Soc. 1993. 34:1–6.25. Cha MB, Min BM, Choi SH. Analysis of ocular motility disturbance remained after open reduction in orbital wall fracture. J Korean Ophthalmol Soc. 1997. 38:1878–1885.
- Full Text Links
-
- Actions
-
Cited
- CITED
-
- Close
- Share
-
- Similar articles
-
- Analysis of Ocular Motility Disturbance remained After Open Reduction in Orbital wall Fracture
- The Postoperative Recovery of Ocular Motility in Pediatric Blow-out Fracture
- Analysis of Ocular Complications and Blowout Fracture in Orbital Blunt Trauma
- Degree of enophthalmos according to the extent of orbital wall fracture and volume of herniated orbital tissue
- The Type of Extraocular Motility Disorder in Blowout Fracture
