Yonsei Med J.
2005 Apr;46(2):233-238. 10.3349/ymj.2005.46.2.233.
Assisted Cough and Pulmonary Compliance in Patients with Duchenne Muscular Dystrophy
- Affiliations
-
- 1Department of Physical Medicine & Rehabilitation, Rehabilitation Institute of Muscular Disease, Yongdong Severance Hospital, Yonsei University College of Medicine, Seoul, Korea. kswoong@yumc. yonsei.ac.kr
- KMID: 1734049
- DOI: http://doi.org/10.3349/ymj.2005.46.2.233
Abstract
- The aim of this study was to investigate the factors affecting cough ability, and to compare the assisted cough methods in patients with Duchenne muscular dystrophy (DMD). A total seventy-one male patients with DMD were included in the study. The vital capacity (VC) and maximum insufflation capacity (MIC) were measured. The unassisted peak cough flow (UPCF) and three different techniques of assisted peak cough flow were evaluated. UPCF measurements were possible for all 71 subjects. But when performing the three different assisted cough techniques, peak cough flows (PCFs) could be obtained from only 51 subjects. The mean value of MICs (1801+/-780cc) was higher than that of VCs (1502+/-765cc) (p< 0.01). All three assisted cough methods showed a significantly higher value than the unassisted method (F=80.92, p< 0.01). The manual assisted PCF under MIC (MPCFmic) significantly exceeded those produced by manual assisted PCF (MPCF) or PCF under MIC (PCFmic). The positive correlation between the MIC, VC difference (MIC-VC), and the difference between PCFmic and UPCF (PCFmic-UPCF) was seen (r= 0.572, p< 0.01). The preservation of pulmonary compliance is important for the development of an effective cough as well as assisting the compression and expulsive phases. Thus, the clinical importance of the inspiratory phase and pulmonary compliance in assisting a cough should be emphasized.
MeSH Terms
Figure
-
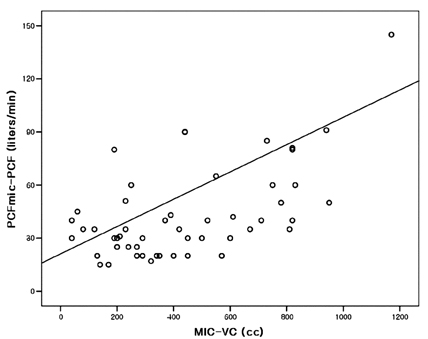
Fig. 1 Relationship between the MIC, VC difference (MIC-VC), and the difference between PCFmic and UPCF (PCFmic-UPCF). The MIC-VC correlated significantly with the PCFmic-UPCF (r=0.572; p < 0.01). MIC, maximum insufflation capacity; VC, vital capacity; PCFmic, peak cough flow under maximum insufflation capacity; UPCF, unassisted peak cough flow.
Cited by 1 articles
-
A Comparison of Cough Assistance Techniques in Patients with Respiratory Muscle Weakness
Sun Mi Kim, Won Ah Choi, Yu Hui Won, Seong-Woong Kang
Yonsei Med J. 2016;57(6):1488-1493. doi: 10.3349/ymj.2016.57.6.1488.
Reference
-
1. Inkley SR, Oldenburg FC, Vignos PJ. Pulmonary function in Duchenne muscular dystrophy related to stage of disease. Am J Med. 1974. 56:297–306.2. Estenne A, Heilporn A, Delhez L, Yernalt JC, Troyer A. Chest wall stiffness in patients with chronic respiratory muscle weakness. Am Rev Respir Dis. 1983. 128:1002–1007.3. Estenne M, Gevenois PA, Kinnear W, Soudon P, Heilporn A, De Troyer A. Lung volume restriction in patients with chronic respiratory muscle weakness: the role of microatelectasis. Thorax. 1993. 48:698–701.4. Suarez AA, Pessolano FA, Monteiro SG, Ferreyra G, Capria ME, Mesa L, et al. Peak flow and peak cough flow in the evaluation of expiratory muscle weakness and bulbar impairment in patients with neuromuscular disease. Am J Phys Med Rehabil. 2002. 81:506–511.5. Scanlan C, Myslinski MJ. Scanlan CL, Wilkins RL, Stoller JK, editors. Bronchial hygiene therapy. Egan's Fundamentals of Respiratory Care. 1999. 7th ed. St. Louis: Mosby;792–793.6. Biering-Sorensen F, Knudsen JL, Schmidt A, Bundgaard A, Christensen I. Effect of respiratory training with a mouth-nose-mask in tetraplegics. Paraplegia. 1991. 29:113–119.7. Estenne M, Knoop C, Vanvaerenbergh J, Heilporn A, De Troyer A. The effect of pectoralis muscle training in tetraplegic subjects. Am Rev Respir Dis. 1989. 139:1218–1222.8. Linder SH. Functional electrical stimulation to enhance cough in quadriplegia. Chest. 1993. 103:166–169.9. Jaeger RJ, Turba RM, Yakony GM, Roth EJ. Cough in spinal cord injured patients: comparison of three methods to produce cough. Arch Phys Med Rehabil. 1993. 74:1358–1361.10. Kang SW, Bach JR. Disorders of ventilation: weakness, stiffness, and mobilization. Chest. 2000. 117:301–303.11. Kang SW, Bach JR. Maximum insufflation capacity: vital capacity and cough flows in neuromuscular disease. Am J Phys Med Rehabil. 2000. 79:222–227.12. Kang SW, Bach JR. Maximum insufflation capacity. Chest. 2000. 118:61–65.13. Kirby NA, Barnerias MJ, Siebens AA. An evaluation of assisted cough in quadriparetic patients. Arch phys Med Rehabil. 1966. 47:705–710.14. Bach JR. Mechanical insufflation-exsufflation. Comparison of peak expiratory flows with manually assisted and unassisted coughing techniques. Chest. 1993. 104:1553–1562.15. Sivasothy P, Brown L, Smith IE, Shneerson JM. Effect of maunally assisted cough and mechanical insufflation on cough flow of normal subjects, patients with chronic obstructive pulmonary disease (COPD), and patients with respiratory muscle weakness. Thorax. 2001. 56:438–444.16. Swinyard CA, Deaver GG. Gradients of functional ability of importance in rehabilitation of patients with progressive muscular and neuromuscular diseases. Arch Phys Med Rehabil. 1957. 38:574–579.17. Morris JF. Spirometry in the evaluation of pulmonary function. West J Med. 1976. 125:110–118.18. DaCosta JL. Pulmonary function studies in healthy Chinese adults in Singapore. Am Rev Respir Dis. 1971. 104:128–131.19. Leith DE. Brain JD, Proctor D, Reid L, editors. Cough. Lung Biology in Health and Disease. 1977. New York: Marcel Dekker;545–592.20. Chatwin M, Ross E, Hart N, Nickol AH, Polkey MI, Simonds AK. Cough augmentation with mechanical insufflation/exsufflation in patients with neuromuscular weakness. Eur Respir J. 2003. 21:502–508.21. Tzeng AC, Bach JR. Prevention of pulmonary morbidity for patients with neuromuscular disease. Chest. 2000. 118:1390–1396.22. McCool FD, Leith DE. Pathophysiology of cough. Clin Chest Med. 1987. 8:189–195.23. Hadjikoutis S, Wiles CM, Eccles R. Cough in motor neuron disease: a review of mechanisms. QJM. 1999. 92:487–494.
- Full Text Links
-
- Actions
-
Cited
- CITED
-
- Close
- Share
-
- Similar articles
-
- Analysis of Pulmonary Mechanics and the Factors for Coughing in Duchenne Muscular Dystrophy
- Clinical Implications of Pulmonary Function Test and Maximum Static Pressure in Duchenne Muscular Dystrophy
- A clinical study on Duchenne muscular dystrophy
- Duchenne Muscular Dystrophy Complicated With Dilated Cardiomyopathy and Cerebral Infarction
- Respiratory Muscle Strength and Cough Capacity in Patients with Duchenne Muscular Dystrophy
