Orbital Apex Syndrome in a Patient with Sphenoid Fungal Balls
- Affiliations
-
- 1Department of Otorhinolaryngology-Head and Neck Surgery, College of Medicine, Hanyang University, Seoul, Korea. shcho@hanyang.ac.kr
- 2Department of Pathology, College of Medicine, Hanyang University, Seoul, Korea. shcho@hanyang.ac.kr
- 3Department of Ophthalmology, College of Medicine, Hanyang University, Seoul, Korea.
- 4Department of Neurosurgery, College of Medicine, Hanyang University, Seoul, Korea.
- KMID: 1466565
- DOI: http://doi.org/10.3342/ceo.2009.2.1.52
Abstract
- Orbital apex syndrome (OAS) is a rare disease that presents with a complex of symptoms, including ophthalmoplegia, ptosis and visual loss. Due to the poor prognosis, making a prompt diagnosis and administering the appropriate treatment must be initiated without delay if OAS is suspected. We report here on a case of a patient with sphenoid fungal balls, and he presented with acute visual loss and ophthalmoplegia.
Keyword
Figure
-
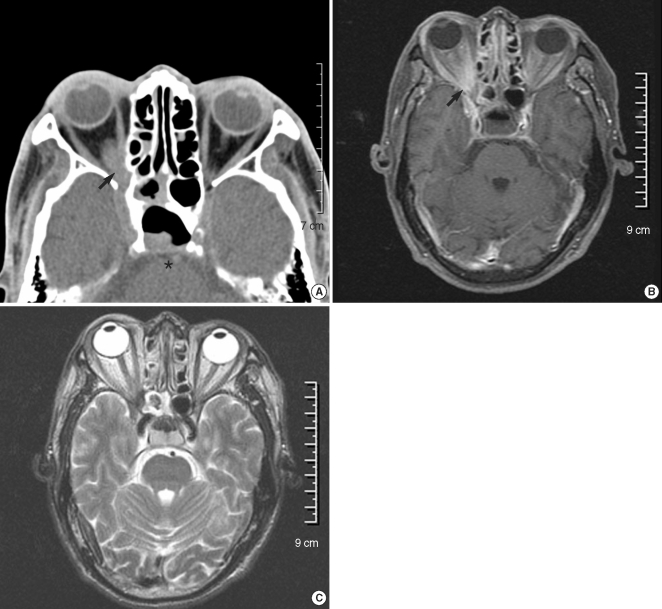
Fig. 1 The orbital CT scan showed soft tissue density at the posterior ethmoid and sphenoid sinuses. The posterior wall of the sphenoid sinus (*) was eroded and the inferior rectus muscle (arrow) was thickened (A). The soft tissue of the sphenoid sinus showed a low-signal on the T1W (B) and an intermediate signal on the T2W (C). Increased signal densities were found at the retrobulbar area and the orbital apex (B, arrow) of the right eye.

Fig. 2 Mucosal biopsy was performed during endoscopic sphenoidotomy. Gomori methenamine silver stain showed minimal tissue invasion of the fungal balls (arrow, ×400).
Cited by 1 articles
-
A Case of Optic Neuropathy Caused by Fungal Ball in an Onodi Cell
Young Soo Han, Chan Min Yang, Jae Ho Shin, In Ki Park
J Korean Ophthalmol Soc. 2014;55(3):426-431. doi: 10.3341/jkos.2014.55.3.426.
Reference
-
1. Yeh S, Foroozan R. Orbital apex syndrome. Curr Opin Ophthalmol. 2004; 12. 15(6):490–498. PMID: 15523194.
Article2. Tarazi AE, Shikani AH. Irreversible unilateral visual loss due to acute sinusitis. Arch Otolaryngol Head Neck Surg. 1991; 12. 117(12):1400–1401. PMID: 1845269.
Article3. Ferguson BJ. Fungus balls of the paranasal sinuses. Otolaryngol Clin North Am. 2000; 4. 33(2):389–398. PMID: 10736412.
Article4. Gungor A, Adusumilli V, Corey JP. Fungal sinusitis: progression of disease in immunosuppression-a case report. Ear Nose Throat J. 1998; 3. 77(3):207–210. 215PMID: 9557411.5. Pieroth L, Winterkorn JM, Schubert H, Millar WS, Kazim M. Concurrent sino-orbital aspergillosis and cerebral nocardiosis. J Neuroophthalmol. 2004; 6. 24(2):135–137. PMID: 15179067.
Article6. Thiagalingam S, Fernando GT, Tan K, O'Donnell BA, Weeks K, Branley M. Orbital apex syndrome secondary to Pseudallescheria boydii fungal sinusitis in an immunocompetent patient. Clin Experiment Ophthalmol. 2004; 10. 32(5):545–547. PMID: 15498073.
- Full Text Links
-
- Actions
-
Cited
- CITED
-
- Close
- Share
-
- Similar articles
-
- A Case of Orbital Apex Syndrome Caused by Mucocele in the Sphenoid Sinus
- Orbital Apex Syndrome Related to Isolated Sphenoid Fungal Sinusitis
- A Case of Rhino-orbital Mucormycoses with Orbital Apex Syndrome in Diabetic Patient
- Three Cases of Fungal Sinusitis with Orbital Complication
- A Case of Multiple Fungal Balls Involving the Isolated Three Sinuses
