Cerebral Air Embolism in a Patient with a Tuberculous-Destroyed Lung during Commercial Air Travel: A Case Report
- Affiliations
-
- 1Department of Radiology, Pusan Paik Hospital, Inje University School of Medicine, Busan, Korea. hwjeong2000@lycos.co.kr
- KMID: 1443471
- DOI: http://doi.org/10.3348/jksr.2011.65.2.109
Abstract
- A cerebral air embolism is a rare cause of stroke, but may occur in patients undergoing invasive cardiac and pulmonary procedures, as well as in divers suffering pulmonary barotrauma from rapid ascent. A cerebral air embolism due to other causes, especially a change of air pressure from air travel, is particularly rare. Here, we report a case of cerebral air embolism during commercial air travel in a patient with an tuberculous-destroyed lung.
MeSH Terms
Figure
-
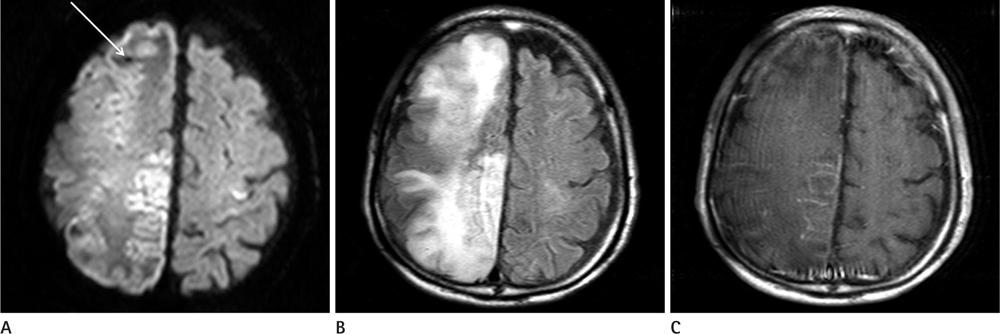
Fig. 1 A. DWI demonstrates acute infarction in the right frontoparietal and left frontal cortical areas and small hypointense lesion in the right frontal area (arrow). B. FLAIR image shows diffuse sulcal effacement and cerebral edema in the right cerebral hemisphere. C. Contrast enhanced T1 weighted image shows multifocal meningeal enhancement in the right frontoparietal lobe. Note.-DWI = diffusion weighted image, FLAIR = fluid attenuated inversion recovery

Fig. 2 A. GRE image shows multifocal hypointense lesions in the right frontoparietal lobe and anterior interhemispheric fissure, some of that, with circumscribed margins (arrow). B. Source image of perfusion CT demonstrates well-defined low attenuated lesion, correspond with well-defined hypointense lesions on GRE, suggesting air embolism (arrow). Note.-GRE = gradient echo image

Fig. 3 A. Chest X-ray in day of admission shows tuberculous-destroyed lung in bilateral upper lung zones with large bullae in the right upper lung zone. B. Source image of anio CT shows tuberculous-destroyed lung in bilateral upper lobe with large bullae in the right upper lobe.
Reference
-
1. Zaugg M, Kaplan V, Widmer U, Baumann PC, Russi EW. Fatal air embolism in an airplane passenger with a giant intrapulmonary bronchogenic cyst. Am J Respir Crit Care Med. 1998; 157:1686–1689.2. Edwardson M, Wurth D, Lacy JM, Fink J, Becker K. Cerebral air embolism resulting in fatal stroke in an airplane passenger with a pulmonary bronchogenic cyst. Neurocrit Care. 2009; 10:218–221.3. Almeida FA, Desouza BX, Meyer T, Gregory S, Greenspon L. Intrapulmonary bronchogenic cyst and cerebral gas embolism in an aircraft flight passenger. Chest. 2006; 130:575–577.4. Salameh J. A 62-year-old woman with cerebral artery air embolism during commercial air travel. Neurologist. 2010; 16:136–137.5. Closon M, Vivier E, Breynaert C, Duperret S, Branche P, Coulon A, et al. Air embolism during an aircraft flight in a passenger with a pulmonary cyst: a favorable outcome with hyperbaric therapy. Anesthesiology. 2004; 101:539–542.6. Neidhart P, Suter PM. Pulmonary bulla and sudden death in a young aeroplane passenger. Intensive Care Med. 1985; 11:45–47.7. Almeida N, Schuller D. Cerebral air embolism resulting from an airplane flight. J Repi Dis. 2007; 28:304–308.8. Oh JY, Park DW, Hahm CK, Park CK, Lee SR, Lee Y. A Cerebral air embolism that developed following defecation in a patient with extensive pulmonary tuberculosis: a case report. J Korean Soc Radiol. 2010; 63:307–310.9. Jeon SB, Kim JS, Lee DK, Kang DW, Kwon SU. Clinicoradio-logical characteristics of cerebral air embolism. Cerebrovasc Dis. 2007; 23:459–462.10. Kang DW, Chalela JA, Ezzeddine MA, Warach S. Association of ischemic lesion patterns on early diffusion-weighted imaging with TOAST stroke subtypes. Arch Neurol. 2003; 60:1730–1734.11. Muth CM, Shank ES. Gas embolism. N Engl J Med. 2000; 342:476–482.
- Full Text Links
-
- Actions
-
Cited
- CITED
-
- Close
- Share
-
- Similar articles
-
- Cerebral Air Embolism Following a Gastroscopy
- Cerebral Air Embolism and Cardiomyopathy Secondary to Large Bulla Rupture during a Pulmonary Function Test
- Stroke Caused by Cerebral Air Embolism after Central Venous Catheter Removal: A Case Report
- Spontaneous Absorption of Cerebral Air Embolus Developed Accidentally during an Intra-arterial Procedure
- A Cerebral Air Embolism That Developed Following Defecation in a Patient with Extensive Pulmonary Tuberculosis: A Case Report
