Idiopathic Synovial Osteochondromatosis of the Hip: Radiographic and MR Appearances in 15 Patients
- Affiliations
-
- 1Department of Radiology, Samsung Medical Center, Sungkyunkwan University School of Medicine, Korea. yspark@smc.samsung.co.kr
- 2Department of Orthopedic Surgery, Samsung Medical Center, Sungkyunkwan University School of Medicine, Korea.
- KMID: 1118793
- DOI: http://doi.org/10.3348/kjr.2002.3.4.254
Abstract
OBJECTIVE
To evaluate the radiographic and MR appearance of idiopathic synovial osteochondromatosis of the hip. MATERIALS AND METHODS: Radiographs and MR images of 15 patients with idiopathic synovial osteochondromatosis of the hip were assessed. The former were analysed in terms of the presence of 1) juxta-articular calcified and/ or ossified bodies, 2) osteophytes, 3) bone erosion, 4) juxta-articular osteopenia, and 5) joint space narrowing, while for the latter, analysis focused on 1) the configuration of intra-articular bodies, 2) bone erosion, 3) synovial thickening, 4) conglomeration of intra-articular bodies, and 5) extra-articular extension. RESULTS: At hip radiography, juxta-articular calcified and/ or ossified bodies were seen in 12 of the 15 patients (80%), bone erosion in eight (53%), osteophytes in seven (47%), juxta-articular osteopenia in five (33%) and joint space narrowing in five (33%). In eight patients (53%), MR imaging depicted intra-articular bodies of focal low signal intensity at all pulse sequences, and areas of isointensity at T1WI and hyperintensity at T2WI. In three (20%), intra-articular bodies of focal low signal intensity and areas of hyperintensity at all pulse sequences were observed, with areas of iso-intensity at T1WI and hyperintensity at T2WI, while in four (27%), intra-articular bodies of only focal low signal intensity at all pulse sequences were apparent. Synovial thickening was present in 13 patients (87%), bone erosion in 11 (73%), conglomeration of the intra-articular bodies in 11 (73%), and an extra-articular herniation sac in six (40%). CONCLUSION: The most common radiographic finding of synovial osteochondromatosis of the hip was the presence of juxta-articular calcified and/ or ossified bodies. MR imaging depicted intra-articular bodies of focal low signal intensity at all pulse sequences, with areas of iso-intensity at T1WI and hyperintensity at T2WI. In addition, the presence of an extra-articular herniation sac was not uncommon.
MeSH Terms
Figure
-
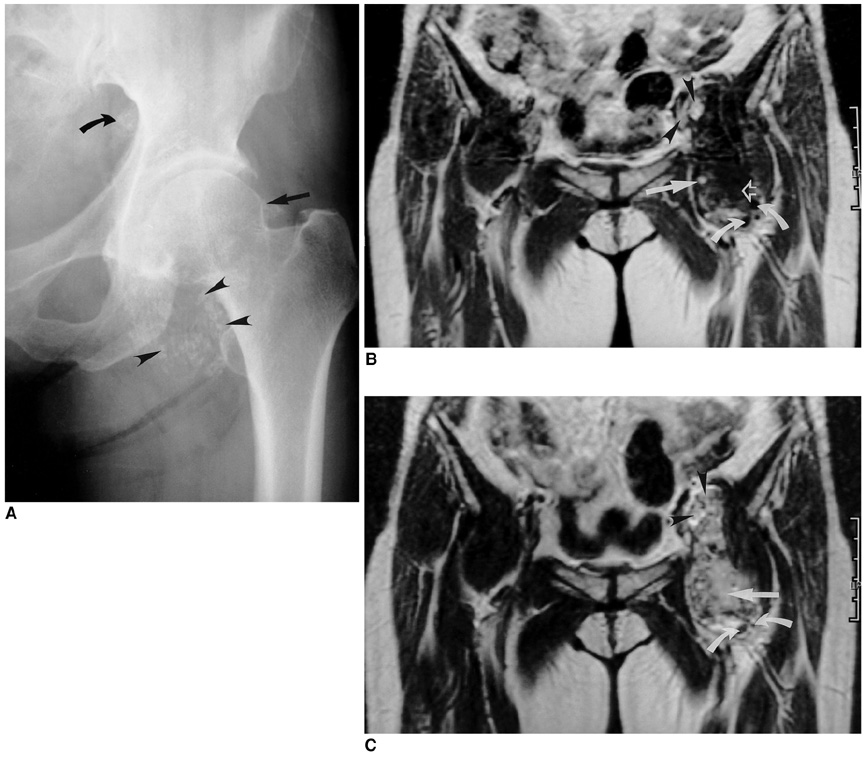
Fig. 1 A 52-year-old woman with idiopathic synovial osteochondromatosis of the left hip. A. Anteoposterior radiograph of the left hip depicts juxta-articular calicified and/ or ossified bodies (arrowheads), and an osteophyte (straight arrow). Note that superior to the iliopubic line, a calcified and/or ossified body (curved arrow) is also present, suggesting intrapelvic extension of the lesion. B. T1-weighted coronal MR image of the same patient shows an intra-articular lesion of low signal intensity (curved arrows), signal intensity which corresponds to an area of fat (straight arrow), and a conglomerated lesion (open arrow). Note that intrapelvic extension of the iliopsoas bursa has occurred (arrowheads). C. T2-weighted image, obtained at the same level as in B, shows intra-articular bodies of focal low signal intensity (curved arrows), and a conglomerated lesion (straight arrow). Note that intrapelvic extension of the iliopsoas bursa is again apparent (arrowheads).

Fig. 2 A 37-year-old man with idiopathic synovial osteochondromatosis of the right hip. A. Anteoposterior radiograph of the right hip demonstrates the presence of juxta-articular calicified and/or ossified bodies (arrowheads), and an osteophyte (arrow). B. T1-weighted axial MR image of the same patient depicts intra-articular bodies of focal low signal intensity (open arrow) and areas of fat (straight arrow). C. T2-weighted image, obtained at the same level as in B, shows intra-articular bodies of focal low signal intensity and central areas of hyaline cartilage (arrows).
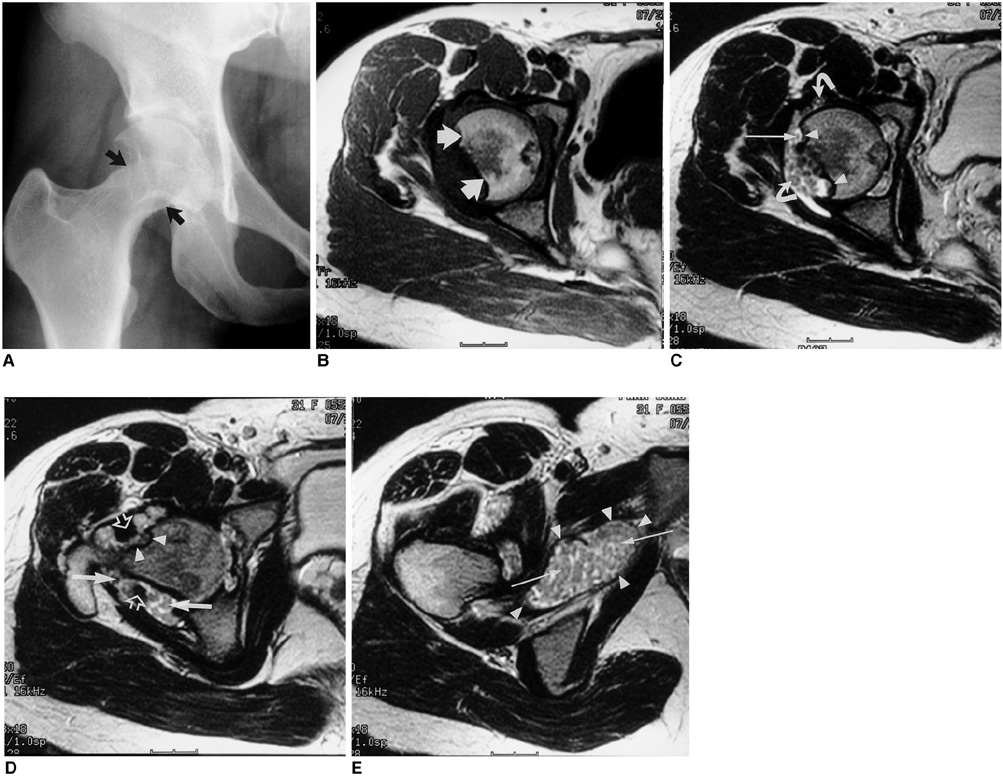
Fig. 3 A 31-year-old woman with idiopathic synovial osteochondromatosis of the right hip. A. Anteoposterior radiograph of the right hip reveals extensive circumferential bone erosion and scalloping of the right femoral neck (arrows). B. T1-weighted axial MR image of the same patient depicts extensive bone erosion (arrows). C. T2-weighted image, obtained at the same level as in B, shows extensive bone erosion (arrowheads), intra-articular bodies without hyaline cartilage or fat (slender arrow), and an intra-articular body with central areas of hyaline cartilage (curved arrows). D. T2-weighted image of the same patient demonstrates extensive bone erosion (arrowheads) around the femoral neck, and the presence of intra-articular bodies (straight arrows). Note that thickening of the synovium (open arrows) has also occurred. E. T2-weighted image of the same patient shows an extra-articular herniation sac (arrowheads) filled with intra-articular bodies (arrows).
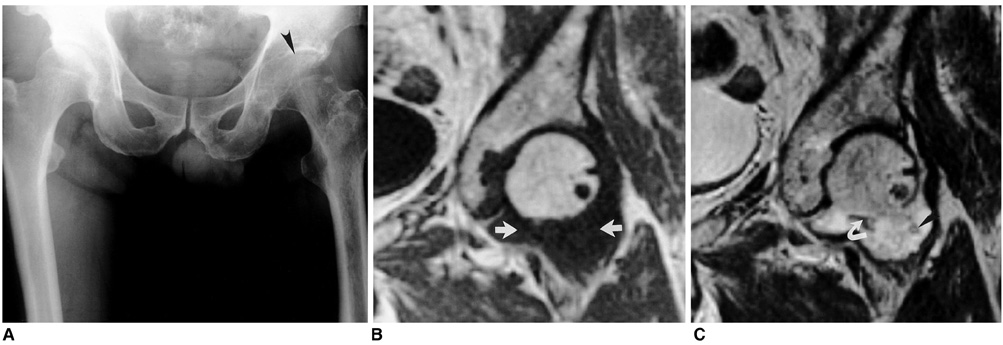
Fig. 4 A 59-year-old man with idiopathic synovial osteochondromatosis of the left hip. A. Anteoposterior radiograph of the left hip shows juxta-articular osteopenia and joint-space narrowing of the left hip joint (arrowhead). B. T1-weighted coronal MR image of the same patient depicts an iso-intense intra-articular lesion (arrows). C. T2-weighted image, obtained at the same level as in B, shows an intra-articular body of low signal intensity (curved arrow). Note that another intra-articular body has peripheral low signal intensity (arrowhead), and the central area has the signal characteristics of hyaline cartilage.
Reference
-
1. Milgram JW. Synovial osteochondromatosis: a histopathological study of thirty cases. J Bone Joint Surg Am. 1977. 59:792–801.2. Kramer J, Recht M, Deely DM, et al. MR appearance of idiopathic synovial osteochondromatosis. J Comput Assist Tomogr. 1993. 17:772–776.3. Llauger J, Palmer J, Roson N, Bague S, Camins A, Cremades R. Nonseptic monoarthritis: imaging features with clinical and histopathologic correlation. RadioGraphics. 2000. 20:S263–S278.4. Norman A, Steiner GC. Bone erosion in synovial chondromatosis. Radiology. 1986. 161:749–752.5. Crotty JM, Monu JUV, Pope TL. Synovial osteochondromatosis. Radiol Clin North Am. 1996. 34:327–342.6. Tuckman G, Wirth CZ. Synovial osteochondromatosis of the shoulder: MR findings. J Comput Assist Tomogr. 1989. 13:360–361.7. Blandino A, Salvi L, Chirico G, et al. Synovialosteochondromatosis of the ankle: MR findings. Clin Imaging. 1992. 16:34–36.8. Vrdoljak J, Irha E. Synovial osteochondromatosis of the sternoclavicular joint. Pediatr Radiol. 2000. 30:181–183.9. Burrafato V, Campanacci DA, Franchi A, Capanna R. Synovial chondromatosis in a lumbar apophyseal joint. Skeletal Radiol. 1988. 27:385–387.10. Mubashir A, Bickerstaff D. Synovial osteochondromatosis of the cruciate ligament. Arthroscopy. 1998. 14:627–629.11. Boles CA, Ward WG. Loose fragments and other debris, miscellaneous synovial and marrow disorders. Magn Reson Imaging Clin N Am. 2000. 8:371–390.12. Peh WCG, Shek TWH, Davies AM, Wong JWK, Chien EP. Osteochondroma and secondary synovial osteochondromatosis. Skeletal Radiol. 1999. 28:169–174.13. Freidman B, Nerubay J, Blankstein A, Kessker A, Horoszowski H. Synovial chondromatosis (osteochondromatosis) of the right hip: hidden radiologic manifestations (case report 439). Skeletal Radiol. 1987. 16:504–508.14. Gilbert SR, Lachiewicz PF. Primary synovial osteochondromatosis of the hip: report of two cases with long-term follow-up after synovectomy and a review of the literature. Am J Orthop. 1997. 26:555–560.15. Pai VR, van Holsbeeck M. Synovial osteochondromatosis of the hip: role of sonography. J Clin Ultrasound. 1995. 23:199–203.16. Friedman B, Caspi I, Nerubay J, Huszar M, Ganel A, Horoszowski H. Synovial chondromatosis of the hip joint. Orthop Rev. 1988. 17:994–998.17. Madewell JE, Sweet DE. Resnick D, editor. Tumors and tumor-like lesions in or about joints. Diagnosis of bone and joint disorders. 1998. 3rd ed. Philadelphia: WB Saunders;3956–3963.18. Bredella MA, Tirman PF, Wischer TK, Belzer J, Taylor A, Genant HK. Reactive synovitis of the knee joint: MR imaging appearance, with arthroscopic correlation. Skeletal Radiol. 2000. 29:577–582.19. Fernandez-Madrid F, Karvonen RL, Teitge RA, Miller PR, Negendank WG. MR features of osteoarthritis of the knee. Magn Reson Imaging. 1994. 12:703–709.20. Villacin AB, Brigham LN, Bullough PG. Primary and secondary synovial chondrometaplasia: histopathologic and clinicoradiologic differences. Hum Pathol. 1979. 10:439–451.21. Sundaram M, McGuire MH, Fletcher J, Wolverson MK, Heiberg E, Shields JB. Magnetic resonance imaging of lesions of synovial origin. Skeletal Radiol. 1986. 15:110–116.
- Full Text Links
-
- Actions
-
Cited
- CITED
-
- Close
- Share
-
- Similar articles
-
- Primary Synovial Osteochondromatosis: A case report
- Synovial Osteochondromatosis of the Cervical Spine: A Case Report
- Synovial Osteochondromatosis of the Subtalar Joint in an Adolescent Baseball Player
- Total Knee Arthroplasty in Severe Synovial Osteochondromatosis in an Osteoarthritic Knee
- The Current Concepts of Hip Arthroscopy
