J Korean Soc Spine Surg.
2014 Dec;21(4):139-145. 10.4184/jkss.2014.21.4.139.
The Analysis of the Outcome of Short- and Long-Segment Posterior Instrumentation for Thoracolumbar Bursting Fractures
- Affiliations
-
- 1Department of Orthopedic Surgery, College of Medicine, Dong-A University, Busan, Korea. gylee@dau.ac.kr
- 2Department of Orthopedic Surgery, Busan Bumin Hospital, Busan, Korea.
- KMID: 2097863
- DOI: http://doi.org/10.4184/jkss.2014.21.4.139
Abstract
- STUDY DESIGN: A retrospective study.
SUMMARY OF THE LITERATURE REVIEW: The reports comparing short- and long-segment instrumentation are insufficient.
OBJECTIVES
To determine the postoperative results and to analyze relative factors affecting results between short- and long-segment instrumentation in thoracolumbar fractures.
MATERIALS AND METHODS
From March 2006 to March 2012, 97 patients with thoracolumbar fracture were treated with posterior instrumentation. They were divided into 2 groups, the short- (Group I) and long-segment groups (Group II). To analyze factors affecting results, several factors including age, anterior column height (ACH), and the kyphotic angle were reviewed. For radiologic evaluation, postoperative and follow-up radiographs were evaluated by measuring the kyphotic angle and ACH. Additionally, the presence of complications was reviewed.
RESULTS
Groups I and II consisted of 45, 52 cases and had mean ages of 50.3, 55.8 years, respectively. In Group I, the ACH increased from 44.2% to 75.3% postoperatively, and remained 72.8% at follow-up. The kyphotic angle decreased from 19.4degrees to 10.6degrees postoperatively, and remained at 12.8degrees at follow-up. In Group II, the ACH recovered from 41.6% to 76.4% postoperatively, and was 74.8% at follow-up. The kyphotic angle decreased from 21.6degrees to 12.6degrees postoperatively, and was 13.9degrees at follow-up. The canal compromise, age, and comminution were not directly related with results. However, the mean age of the 7 cases showing complications was 72 years, and the 7 cases had severe comminuted fractures.
CONCLUSIONS
The short- and long-segment instrumentations of thoracolumbar fractures are not significantly different with respect to the results attained. However, in order to decrease complications, we should pay attention to age and fracture comminution.
Keyword
Figure
-
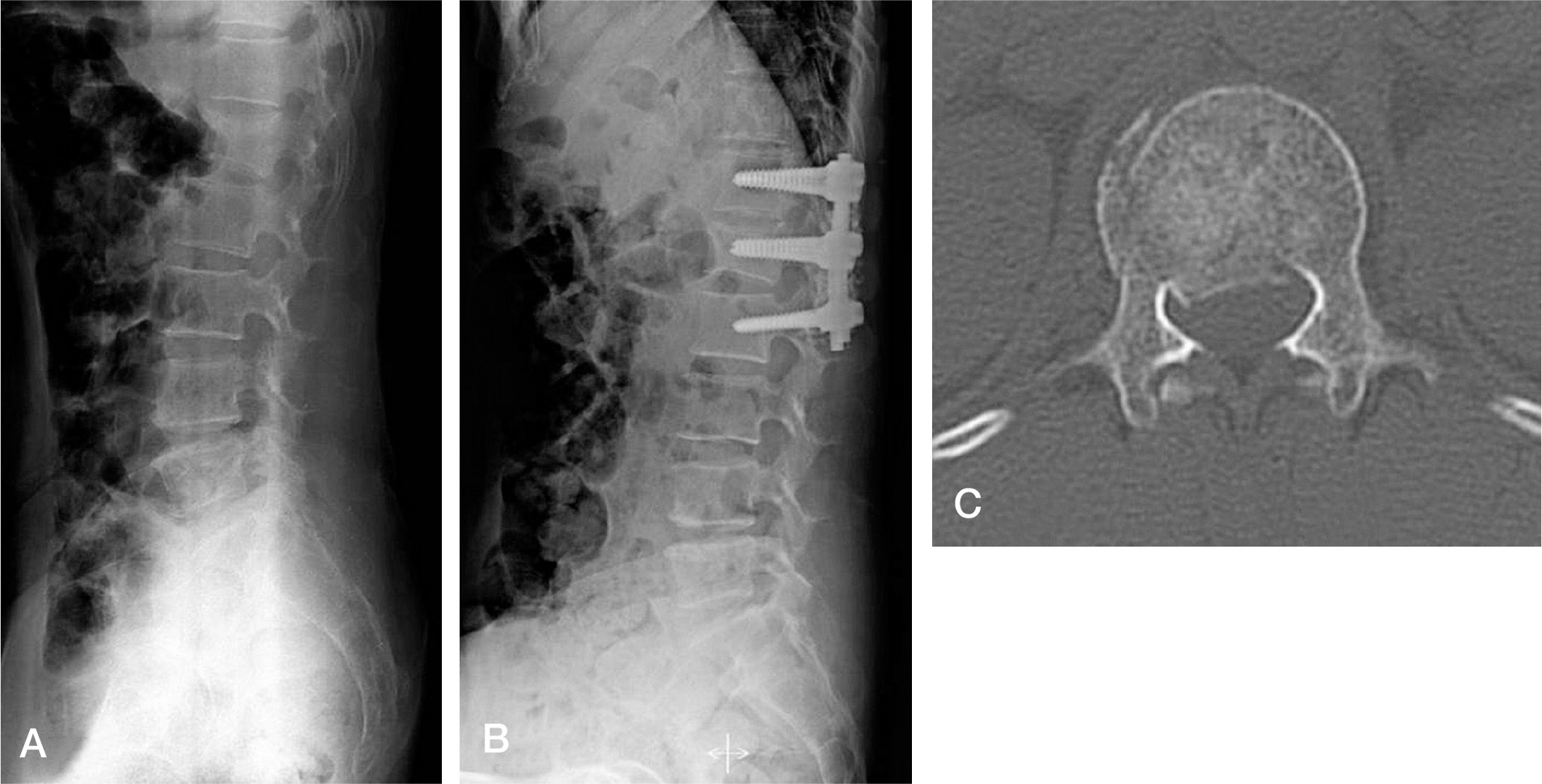
Fig. 1. A 60-year-old female patient with L1 burst fracture treated by short segment pedicle screw fixation. (A) Preoperative X-ray (B) Postoperative X-ray (C) Preoperative CT scan.
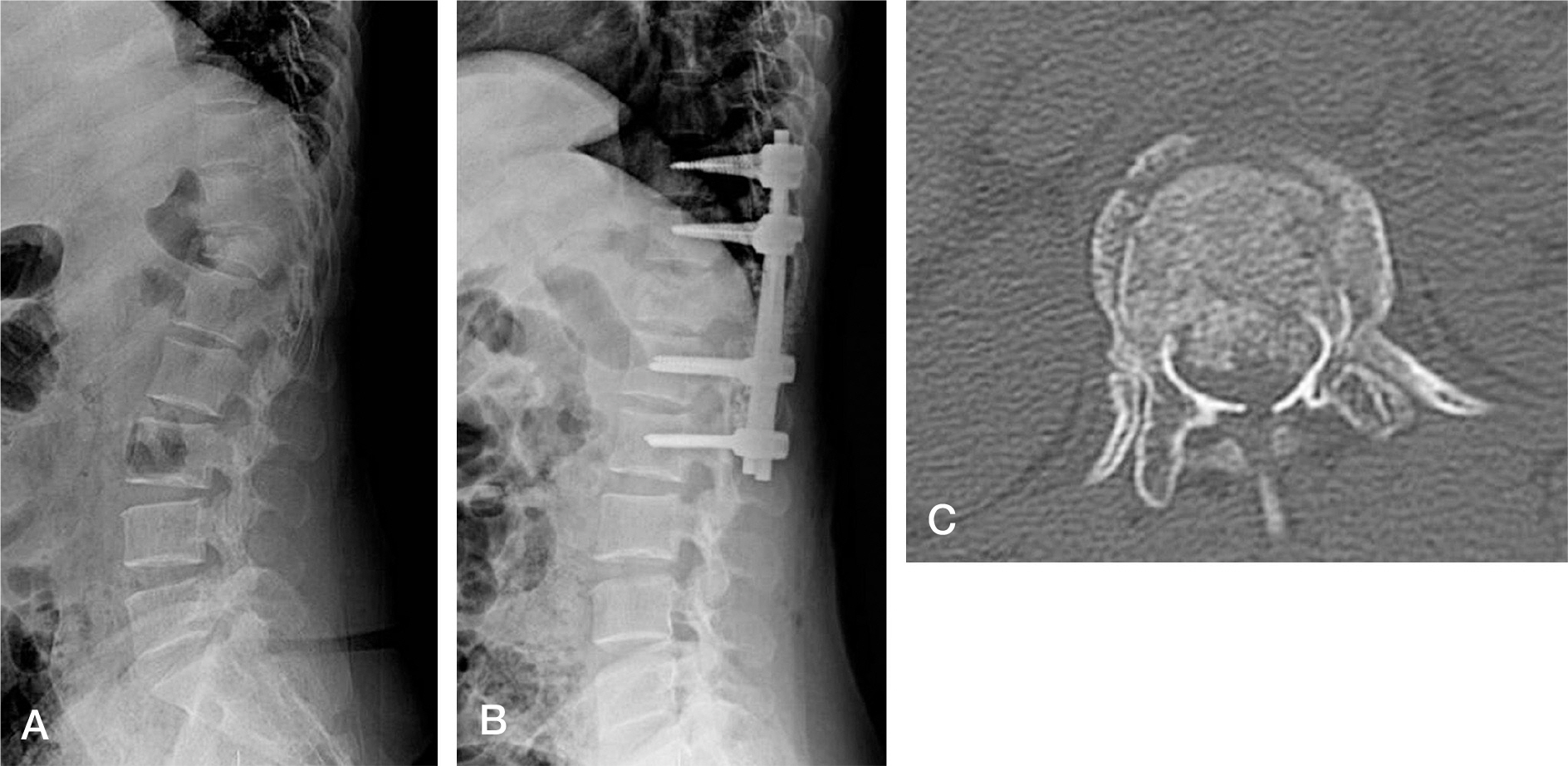
Fig. 2. A 31-year-old female patient with T12 burst fracture treated by long segment pedicle screw fixation. (A) Preoperative X-ray (B) Postoperative X-ray (C) Preoperative CT scan.
Cited by 1 articles
-
The Outcomes of Short and Long Segment Posterior Instrumentation of Thoracolumbar Burst Fractures with a Load Sharing Score of 7 or More
Jeong Ho Seo, Kyu Yeol Lee
J Korean Soc Spine Surg. 2015;22(3):92-98. doi: 10.4184/jkss.2015.22.3.92.
Reference
-
1. Mclain R. The biomechanics of long versus short fixation for thoracolumbar spine fractures. Spine (Phila Pa 1976). 2006; 31:70–9.
Article2. Lee CS, Chung SS, Jung HW, Kim ES. Decision of posterior fixation level by load-sharing classification in thoracolumbar and lumbar burst fracture. J Korean Soc Spine Surg. 2001; 8:27–38.
Article3. Arlet V, Orndorff DG, Jagannathan J, Dumont A. Reverse and pseudoreverse cortical sign in thoracolumbar burst fracture: radiologic description and distinction-a propos of three cases. Eur Spine J. 2009; 18:282–7.
Article4. Cortrel Y, Dubousset J, Guillaumat M. New universal instrumentation in spinal surgery. Clin Orthop. 1988; 227:10–23.5. Roy-Camille R, Saillant G, Mazel C. Internal fixation of the lumbar spine with pedicle screw plating. Clin Orthop. 1986; 203:7–17.
Article6. Steffee AD, Biscup RS, Sitkowski DJ. Segmental spine plates with pedicle screw fixation. A new internal fixation device for disorder of the lumbar and thoracolumbar spine. Clin Orthop. 1986; 203:45–53.7. Been HD, Bouma GJ. Comparison of two types of surgery for thoracolumbar burst fractures: combined anterior and posterior stabilization vs. posterior instrumentation only. Neurochirugica. 1999; 141:349–57.8. Sjostrom L, Jakobsson O, Karlstrom G, Pech P, Rauschning W. Spinal canal remodeling after stabilization of thoracolumbar burst fractures. Eur Spine J. 1994; 3:312–7.9. Sjostrom L, Karlstrom G, Pech P, Rauschning W. Indi-rect spinal canal decompression in burst fractures treated with pedicle screw instrumentation. Spine (Phila Pa 1976). 1996; 21:113–23.10. Esses SI, Botsford DJ, Kostuik JP. Evaluation of surgical treatment for burst fractures. Spine (Phila Pa 1976). 1990; 15:667–73.
Article11. McLain RF, Sparling E, Benson DR. Early failure of short segment pedicle instrumentation for thoracolumbar fractures. J Bone Joint Surg. 1993; 75:162–7.12. Shono Y, McAfee PC, Cunningham BW. Experimental study of thoracolumbar burst fractures. Spine (Phila Pa 1976). 1994; 19:1711–22.
Article13. Zindrick MR. The role of transpedicular fixation system for stabilization of the lumbar spine. Orthop Clin N Am. 1991; 2:333–43.14. Holt BT, McCormack T, Gaines RW. Short segment fusion – anterior or posterior approach? The load-sharing classification of spinal fractures. Spine (Phila Pa 1976). 1993; 7:277–85.15. Robert FM, Edward S, Daniel RB. Early failure of short segment pedicle instrumentation for thoracolumbar fractures. J Bone Joint Surg. 1993; 75:162–7.16. McCormack T, Karaikovic E, Gaines RW. The load sharing classification of spine fractures. Spine (Phila Pa 1976). 1994; 19:1741–4.
Article17. Lee YS, Sung JK. Longterm Followup Results of Short-segment Posterior Screw Fixation for Thoracolumbar Burst Fractures. J Korean Neurosurg Soc. 2005; 37:416–21.18. Chung JY, Rhym IS. Short segment transpedicular Cotrel-Dubousset instrumentation including involved vertebra for fractures of thoracic and lumbar spine. J Korean Orthop Assoc. 1994; 29:940–8.
Article19. Wei FX, Liu SY, Liang CX, et al. Transpedicular fixation in management of thoracolumbar burst fractures: monosegmental fixation versus short-segment instrumentation. Spine (Phila Pa 1976). 2010; 35:714–20.20. Willen J, Anderson J, Toomoka K, Singer K. The natural history of burst fractures at the thoracolumbar junction. J spinal disorders. 1990; 3:39–46.
Article21. Pau A, Silvestro C, Carta F. Can lacerations of the thoracolumbar dura be predicteed on the basis of radiological patterns of the spinal fractures? Acta Neurochir. 1994; 129:186–7.22. Silvestro C, Francaviglia N, Bragazzi R, Piatelli G, Viale GL. On the predictive value of radiological signs for the presence of dural lacerations related to fractures of the lower thoracic or lumbar spine. J Spinal Disord. 1991; 4:49–53.23. Haluk A, Kayali C, Arslantas M. Nonoperative treatment of burst-type thoracolumbar vertebra fractures: clinical and radiological results of 29 patients. Eur Spine J. 2005; 14:536–40.
Article24. Jeong ST, Cho SH, Song HR, Koo KH, Park HB, Chung UH. Comparison of short and long segment fusion in thoracic and lumbar fracture. J Korean Spine Surg. 1999; 6:73–80.
- Full Text Links
-
- Actions
-
Cited
- CITED
-
- Close
- Share
-
- Similar articles
-
- The Outcomes of Short and Long Segment Posterior Instrumentation of Thoracolumbar Burst Fractures with a Load Sharing Score of 7 or More
- Comparison of Short Segment and Long Segment Posterior Instrumentation of Thoracolumbar and Lumbar Bursting Fractures at Load Sharing Score 7 or Above
- The Analysis of the Outcome of Short- and Long-Segment Posterior Instrumentation for Thoracolumbar Bursting Fractures
- Short Segment versus Long Segment Pedicle Screws Fixation in Management of Thoracolumbar Burst Fractures: Meta-Analysis
- Treatment of Thoraco-Lumbar Bursting Fractures According to Load-Sharing Classification
