Biportal Endoscopic Spinal Surgery for Recurrent Lumbar Disc Herniations
- Affiliations
-
- 1Spine Center, BESS Education Center, Barun Hospital, Jinju, Korea. djchoi9@hanmail.net
- 2Department of Orthopaedics, Barun Hospital, Seoul, Korea.
- KMID: 2374280
- DOI: http://doi.org/10.4055/cios.2016.8.3.325
Abstract
- The major problems of revision surgery for recurrent lumbar disc herniation (LDH) include limited visualization due to adhesion of scar tissue, restricted handling of neural structures in insufficient visual field, and consequent higher risk of a dura tear and nerve root injury. Therefore, clear differentiation of neural structures from scar tissue and adhesiolysis performed while preserving stability of the remnant facet joint would lower the risk of complications and unnecessary fusion surgery. Biportal endoscopic spine surgery has several merits including sufficient magnification with panoramic view under very high illumination and free handling of instruments normally impossible in open spine surgery. It is supposed to be a highly recommendable alternative technique that is safer and less destructive than the other surgical options for recurrent LDH.
Keyword
MeSH Terms
Figure
-

Fig. 1 Preparation of the procedure. (A) The position of the patient with the back flat, the head down and the hip flexed. (B) The target point of spinal needle insertion for dyeing of the disc. (C) Biportal inlets were located over the margin of the interlaminar space rather than the level of disc space.
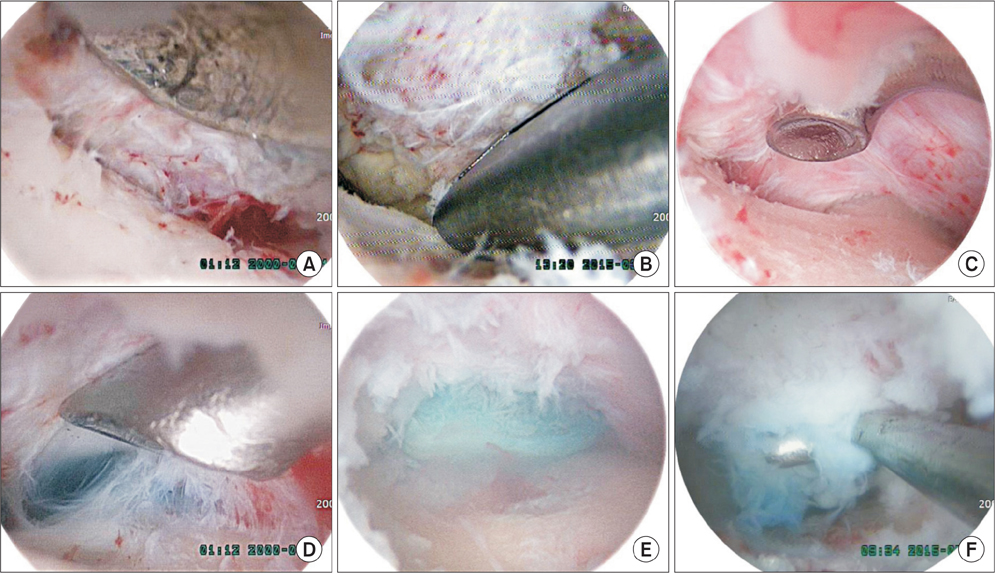
Fig. 2 Revision biportal endoscopic spine surgery. (A) With the bony margin of the facet exposed, adhesiolysis of scar tissue was safely performed from the bony tissue of the lamina under excellent magnification and bright illumination with curetting to differentiate it from soft tissue scar. (B) Decompression somewhat wider with a Kerrison punch to make a room for inspecting the disc space. (C) Probing and searching the disc space along the bony margin of the pedicle to the base. (D) Stained basal area indicated the ruptured disc level. (E) The ruptured disc fragment stained by indigo carmine was exposed at the ruptured site. (F) The ruptured fragment was removed by a hook.
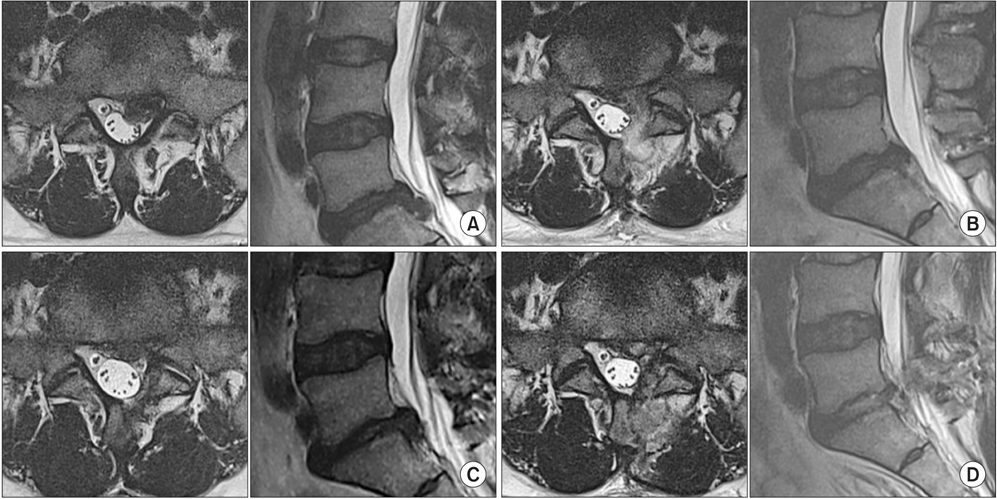
Fig. 3 A 43-year-old male patient with recurring lumbar disc herniation (LDH) at L5–S1. (A) Magnetic resonance imaging (MRI) scans of the ruptured disc in the first event. (B) Postoperative axial MRI scans after open microdiscectomy. (C) Axial and sagittal views of the recurring LDH at 7 months after the first operation. (D) Postoperative MRI scans after the revision surgery: biportal endoscopic spine surgery with decompression of the affected disc and preservation of the facet.
Cited by 4 articles
-
Unilateral Biportal Endoscopic Spinal Surgery Using a 30° Arthroscope for L5–S1 Foraminal Decompression
Ju-Eun Kim, Dae-Jung Choi
Clin Orthop Surg. 2018;10(4):508-512. doi: 10.4055/cios.2018.10.4.508.Clinical and Radiological Outcomes of Foraminal Decompression Using Unilateral Biportal Endoscopic Spine Surgery for Lumbar Foraminal Stenosis
Ju-Eun Kim, Dae-Jung Choi, Eugene J. Park
Clin Orthop Surg. 2018;10(4):439-447. doi: 10.4055/cios.2018.10.4.439.Efficacy of Biportal Endoscopic Spine Surgery for Lumbar Spinal Stenosis
Dae-Jung Choi, Ju-Eun Kim
Clin Orthop Surg. 2019;11(1):82-88. doi: 10.4055/cios.2019.11.1.82.Biportal Endoscopic Spinal Surgery for Lumbar Intervertebral Disc Herniation
Lee Ho-Jin, Choi Dae-Jung, J. Park Eugene
J Korean Orthop Assoc. 2019;54(3):211-218. doi: 10.4055/jkoa.2019.54.3.211.
Reference
-
1. Kim MS, Park KW, Hwang C, et al. Recurrence rate of lumbar disc herniation after open discectomy in active young men. Spine (Phila Pa 1976). 2009; 34(1):24–29.
Article2. Oh JT, Park KS, Jung SS, et al. Surgical results and risk factors for recurrence of lumbar disc herniation. Korean J Spine. 2012; 9(3):170–175.
Article3. Hou T, Zhou Q, Dai F, et al. Repeated microendoscopic discectomy for recurrent lumbar disk herniation. Clinics (Sao Paulo). 2015; 70(2):120–125.
Article4. Shin KH, Chang HG, Rhee NK, Lim KS. Revisional percutaneous full endoscopic disc surgery for recurrent herniation of previous open lumbar discectomy. Asian Spine J. 2011; 5(1):1–9.
Article5. El Shazly AA, El Wardany MA, Morsi AM. Recurrent lumbar disc herniation: a prospective comparative study of three surgical management procedures. Asian J Neurosurg. 2013; 8(3):139–146.
Article6. Choi CM, Chung JT, Lee SJ, Choi DJ. How I do it? Biportal endoscopic spinal surgery (BESS) for treatment of lumbar spinal stenosis. Acta Neurochir (Wien). 2016; 158(3):459–463.
Article7. Soliman HM. Irrigation endoscopic discectomy: a novel percutaneous approach for lumbar disc prolapse. Eur Spine J. 2013; 22(5):1037–1044.
Article
- Full Text Links
-
- Actions
-
Cited
- CITED
-
- Close
- Share
-
- Similar articles
-
- Complications and Management of Endoscopic Spinal Surgery
- Percutaneous Endoscopic Lumbar Discectomy (PELD)
- Biportal Endoscopic Spinal Surgery for Recurrent Lumbar Disc Herniations
- Biportal Endoscopic Transforaminal Lumbar Interbody Fusion with Arthroscopy
- Removal of Lumbar Synovial Cyst Using Biportal Endoscopic Surgery: A Case Report
