The Analysis of Prognostic Factors on Unstable Burst Fracture on the Thoracolumbar Spine
- Affiliations
-
- 1Department of Orthopedic Surgery, College of Medicine, Dong-A University, Busan, Korea. tynitus@dau.ac.kr
- KMID: 1473383
- DOI: http://doi.org/10.4184/jkss.2009.16.1.1
Abstract
-
STUDY DESIGN: A retrospective clinical and radiological analysis
OBJECTIVES
To determine the relationship between the classifications of unstable burst fractures on the thoracolumbar region, radiologic studies, signal change area on MRA and analysis of the prognostic factors. SUMMARY OF LITERATURE REVIEW: MRI is the first imaging modality that visualizes the extent of spinal cord derangement directly and it has the potential to provide an accurate diagnosis and prognosis.
MATERIALS AND METHODS
From March 1998 to September 2006, 39 patients who were eligible for a follow up of more than 1 year with an unstable burst fracture on the thoracolumbar region were studied. With these cases, The size of the bone fragment at the initial injury, signal change area on MRI, time to surgery, reduction rate of the bone fragments, recovery of the posterior curvature of the vertebrae and height of the vertebral body were analyzed.
RESULTS
The mean fracture size rate, average time to surgery, reduction rate of bone fragment and the recovery rate of the height of the vertebral body was 46.1+/-12.8%, 17+/-4.5 hours, 35.2+/-10.1%, and 57.9+/-17.4%, respectively. The data shows that the time elapsed until surgery had no relationship with the prognosis (P=0.317). Injuries with broad signal changes on MRI were not associated with the reduction rate of bone fragments, recovery of posterior curvature of the vertebrae and the height of the vertebral body.
CONCLUSIONS
In unstable burst fractures of the thoracolumbar region, although a comparison of the prognostic factors on simple X-ray film had no significance, it still has significant meaning when correlated with the signals on MRI.
Figure
-
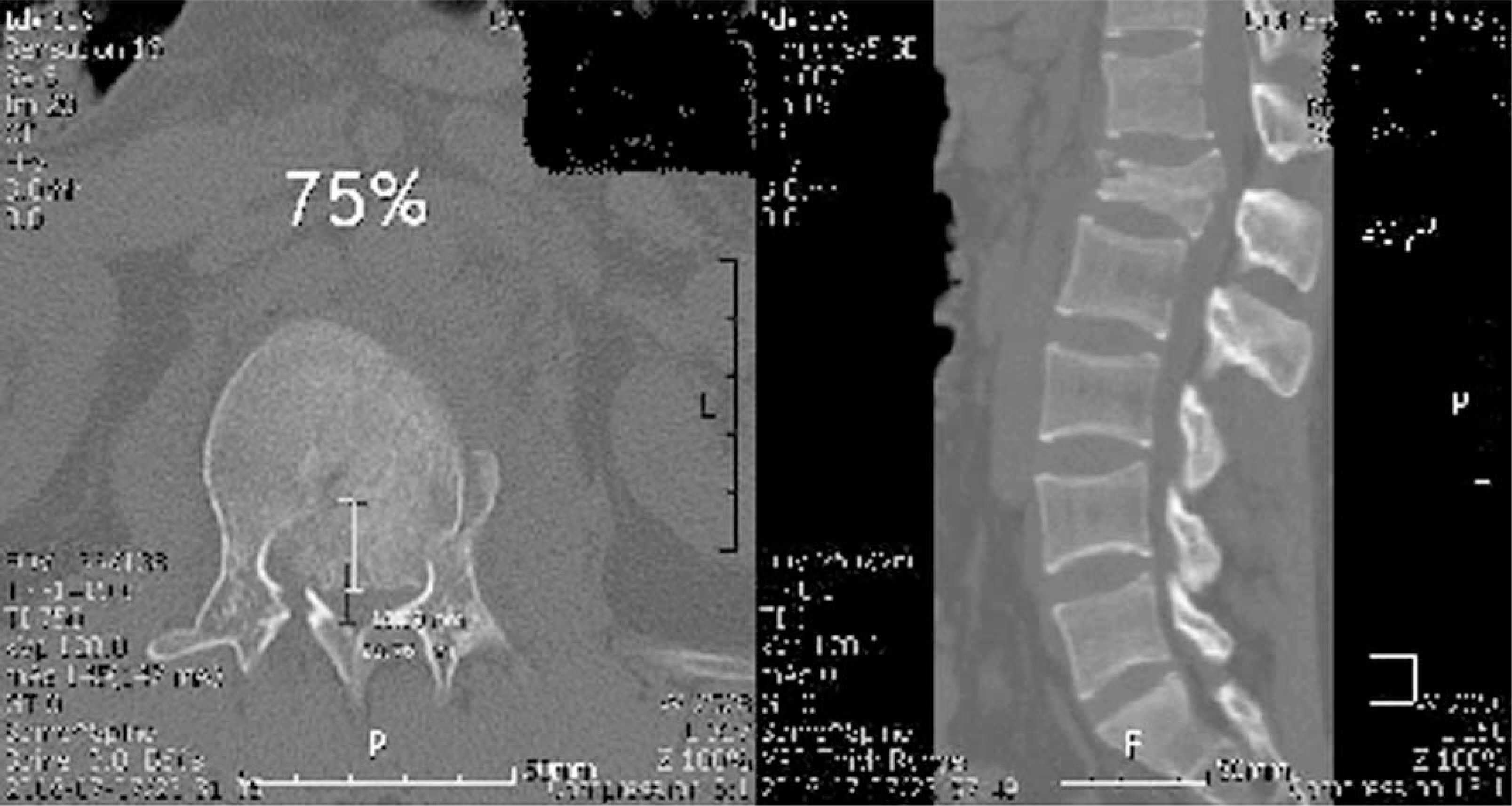
Fig. 1. CT scan shows retropulsed fragment into the spinal canal.
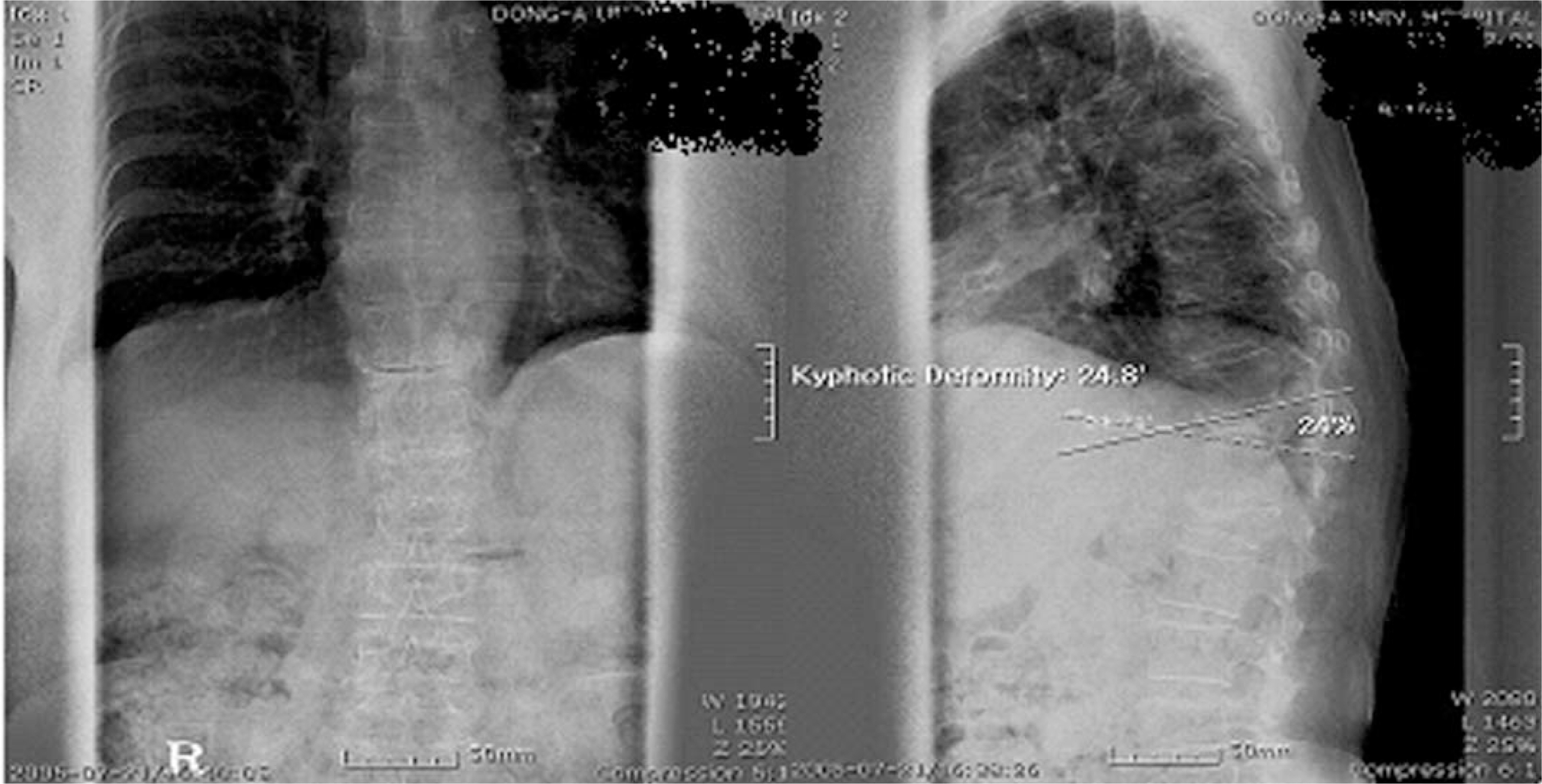
Fig. 2. AP and lateral views of preoperative state, kyphotic angle was 24.8 degrees, reserver rate was 24%.
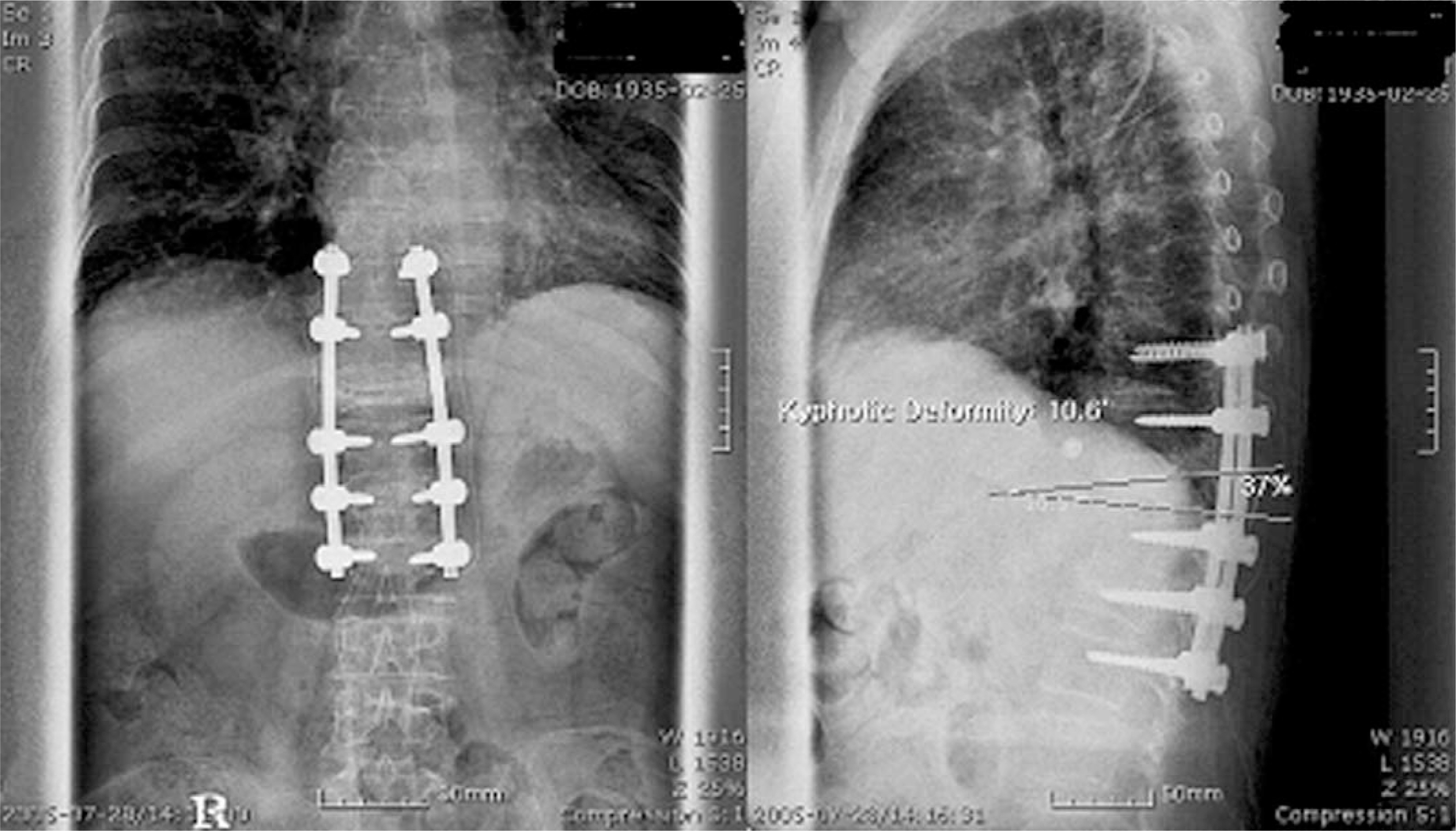
Fig. 3. Immediately postoperative state, kyphotic angle was 10.6 degrees, reserver rate was 37%.
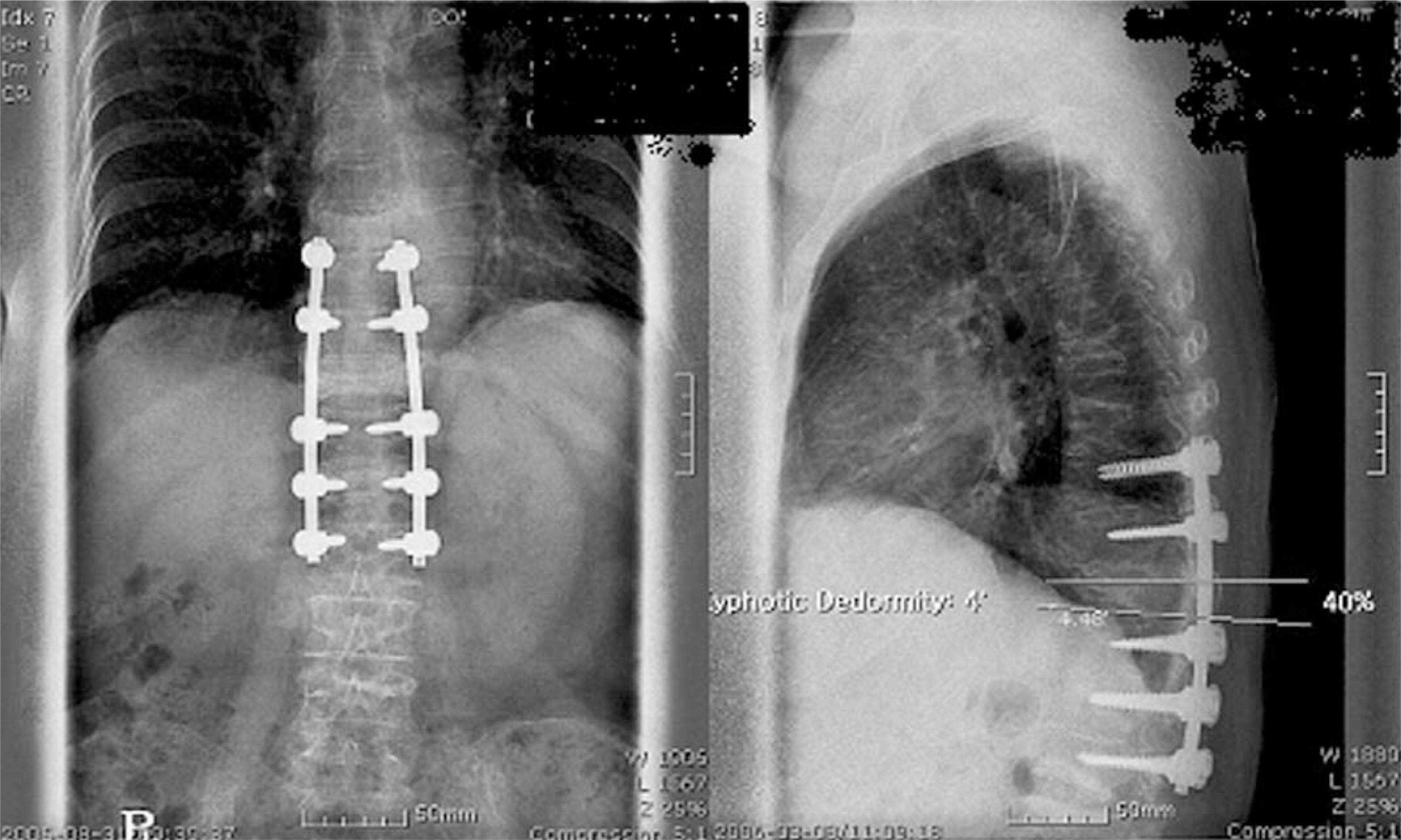
Fig. 4. Six months after operation, kyphotic angle was 4 degrees, reserver rate was 40%.

Fig. 5. Quantitative analysis of signal changes on MRI.
Cited by 2 articles
-
Comparison of TLICS & McAfee Classification in Thoracolumbar Injuries
Woo Chul Kim, Kyu Yeol Lee, Jin Hun Kang, Young Hoon Lim
J Korean Soc Spine Surg. 2012;19(1):8-15. doi: 10.4184/JKSS.2021.19.1.8.Conus Medullaris Syndrome Caused by Delayed Recollapse after Surgery of Burst Fracture - A Case Report -
Jae-Wan Soh, Jae Chul Lee, Jung-Moo Seo, Byung-Joon Shin
J Korean Soc Spine Surg. 2014;21(3):129-133. doi: 10.4184/jkss.2014.21.3.129.
Reference
-
01). Kim YT., Lee CS., Kim CH., Joo DM. Surgical treatment of unstable thoracolumbar fractures with posterior approach. J. of Korean Orthop. Assoc. 1996. 34:651–656.02). Willen J., Anderson J., Toomoka K., Singer K. The natural history of burst fractures at the thoracolumbar junction. J spinal disorders. 1990. 3:39–46.
Article03). Bohlman HH., Kirkpatrick JS., Delamarter RB., Leventhal M. Anterior decompression for late pain and paralysis after fractures of the thoracolumbar spine. Clin Orthop. 1994. 300:24–29.
Article04). Tasdemiroglu E., Tibbs PA. Long-term follow-up results of thoracolumbar fractures after posterior instrumentation. Spine. 1995. 20:1704–1718.
Article05). Yoon HK., Jeon HS., Cho KN., Kang SI. Prognotic factors to final results after conservative or Surgical treatment of thoracolumbar burst fractures. J. of Korean Spine Surg. 1998. 5:215–223.06). Chung JH., Yoon SH., Park HC., Park CO., Kim EY., Ha Y. Analysis of factors related to neurological deficit in thoracolumbar fractures. J Korean Neurosurg. 2007. 41:1–6.07). Haluk Agus, C. Kayali, M. Arslantas. Nonoperative treatment of burst-type thoracolumbar vertebra fractures: clinical and radiological results of 29 patients. Eur Spine J. 2005. 14:536–540.08). Carl AL., Mstsumoto M., Whalen JT. Anterior dural laceration caused by thoracolumbar and lumbar burst fractures. J Spinal Disord. 2000. 13:399–403.
Article09). Keenen TL., Antony J., Benson DR. Dural tears associated with lumbar burst fractures. J Ortho Trauma. 1990. 4:243–245.
Article10). Aydinli U., Karaeminogullari O., Tiskaya K., Ozturk C. Dural tears in lumbar burst fractures with greenstic lamina fracture. Spine. 2001. 26:410–415.11). Pau A., Silvestro C., Carta F. Can lacerations of the thoracolumbar dura be predicteed on the basis of radiological patterns of the spinal fractures? Acta Neurochir. 1994. 129:186–187.12). Silvestro C., Francaviglia N., Bragazzi R., Piatelli G., Viale GL. On the predictive value of radiological signs for the presence of dural lacerations related to fractures of the lower thoracic or lumbar spine. J Spinal Disord. 1991. 4:49–53.
- Full Text Links
-
- Actions
-
Cited
- CITED
-
- Close
- Share
-
- Similar articles
-
- The Analysis of Prognostic Factors on Unstable Burst Fracture on the Thoracolumbar Spine
- A Clinical Study of Unstable Fractures and Fracture-Dislocations of the Thoracolumbar Spine - Comparision Between Holdsworth, Denis and McAfee Classification -
- Comparative Study of Radiologic Changes after Conservative Treatment in Compression fracture and Stable Bursting Fracture of Thoracolumbar Spine
- Crush-Cleavage Fracture in Thoracolumbar and Lumbar Spine: Comparative Study with Type B Burst Fracture
- Assessment of Operative Reduction in Thoracolumbar and Lumbar Spine Fractures
