Yonsei Med J.
2009 Oct;50(5):732-735. 10.3349/ymj.2009.50.5.732.
Intestinal Endometriosis Mimicking Carcinoma of Rectum and Sigmoid Colon: A Report of Five Cases
- Affiliations
-
- 1Department of Surgery, Yonsei University College of Medicine, Seoul, Korea. namkyuk@yuhs.ac
- 2Department of Pathology, Yonsei University College of Medicine, Seoul, Korea.
- KMID: 1103833
- DOI: http://doi.org/10.3349/ymj.2009.50.5.732
Abstract
- Among women with intestinal endometriosis, the sigmoid colon and rectum are the most commonly involved areas. Sometimes, the differential diagnosis of colorectal endometriosis from carcinoma of the colon and rectum is difficult due to similar colonoscopic and radiologic findings. From October 2002 to September 2007, we performed five operations with curative intent for rectal and sigmoid colon cancer that revealed intestinal endometriosis. Colonoscopic and radiologic findings were suggestive of carcinoma of rectum and sigmoid colon, such as rectal cancer, sigmoid colon cancer and gastrointestinal stromal tumor (GIST). Anterior resection was performed in two patients, low anterior resection was performed in one patient and laparoscopic low anterior resection was done in two patients. We suggest to consider also intestinal endometriosis in reproductive women presenting with gastrointestinal symptoms and an intestinal mass of unknown origin.
MeSH Terms
Figure
-
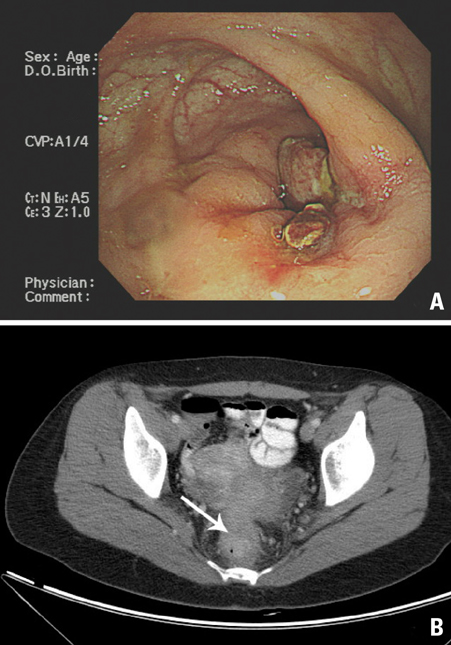
Fig. 1 (A) Colonoscopic finding. Ulcerofungating mass 8 cm above the anal verge is suspicious for rectal cancer. (B) CT scan of the pelvis shows rectal mass with perirectal tumor infiltration (Case 2).

Fig. 2 (A) Gross specimen. The polypoid mass is seen on the laparoscopically resected rectum. (B) The mass was revealed as endometriosis, which is composed of stroma and glands of endometrium, upon microscopic analysis (Hematoxylin Eosin×100) (Case 5).
Cited by 1 articles
-
A Patient with Hematochezia and Intestinal Obstruction
Kyong Yong Oh, Yoon Jae Kim
Intest Res. 2014;12(3):256-257. doi: 10.5217/ir.2014.12.3.256.
Reference
-
1. Olive DL, Schwartz LB. Endometriosis. N Engl J Med. 1993. 328:1759–1769.
Article2. Croom RD 3rd, Donovan ML, Schwesinger WH. Intestinal endometriosis. Am J Surg. 1984. 148:660–667.
Article3. Miller LS, Barbarevech C, Friedman LS. Less frequent causes of lower gastrointestinal bleeding. Gastroenterol Clin North Am. 1994. 23:21–52.
Article4. Giudice LC, Kao LC. Endometriosis. Lancet. 2004. 364:1789–1799.
Article5. Barclay RL, Simon JB, Vanner SJ, Hurlbut DJ, Jeffrey JF. Rectal passage of intestinal endometriosis. Dig Dis Sci. 2001. 46:1963–1967.6. Langlois NE, Park KG, Keenan RA. Mucosal changes in the large bowel with endometriosis: a possible cause of misdiagnosis of colitis? Hum Pathol. 1994. 25:1030–1034.
Article7. Dimoulios P, Koutroubakis IE, Tzardi M, Antoniou P, Matalliotakis IM, Kouroumalis EA. A case of sigmoid endometriosis difficult to differentiate from colon cancer. BMC Gastroenterol. 2003. 3:18.
Article8. Brosens I, Puttemans P, Campo R, Gordts S, Brosens J. Non-invasive methods of diagnosis of endometriosis. Curr Opin Obstet Gynecol. 2003. 15:519–522.
Article9. Mahutte NG, Arici A. Medical management of endometriosis-associated pain. Obstet Gynecol Clin North Am. 2003. 30:133–150.
Article10. Emmanuel KR, Davis C. Outcomes and treatment options in rectovaginal endometriosis. Curr Opin Obstet Gynecol. 2005. 17:399–402.
Article
- Full Text Links
-
- Actions
-
Cited
- CITED
-
- Close
- Share
-
- Similar articles
-
- Intestinal Endometriosis Mimicking Carcinoma of Rectum and Sigmoid Colon: A Report of Five Cases
- Descending Colon Endometriosis Misdiagnosed as Diverticulitis: A Case Report
- A case of bowel obstruction due to endometriosis
- Hirschsprung's Disease Associated with Neonatal Intestinal Perforation
- Endometrial Stromal Sarcoma of the Sigmoid Colon Arising in Endometriosis :A Case Report with a Review of Literatures
