The Stent-Assisted Coil-Jailing Technique Facilitates Efficient Embolization of Tiny Cerebral Aneurysms
- Affiliations
-
- 1Department of Neurosurgery, Shijiazhuang First Hospital, Hebei Medical University, Shijiazhuang 050011, China. browngao@163.com
- KMID: 1794659
- DOI: http://doi.org/10.3348/kjr.2014.15.6.850
Abstract
OBJECTIVE
Tiny cerebral aneurysms are difficult to embolize because the aneurysm's sac is too small for a single small coil, and coils within the aneurysm may escape from the confinement of a stent. This study was performed to introduce the stent-assisted coil-jailing technique and to investigate its effect on the coil embolization of tiny intracranial aneurysms.
MATERIALS AND METHODS
Sixteen patients with tiny intracranial aneurysms treated with the stent-assisted coil-jailing technique between January 2011 and December 2013 were retrospectively reviewed and followed-up.
RESULTS
All aneurysms were successfully treated with the coil-jailing technique, and at the end of embolization, complete occlusion of the aneurysm was achieved in 9 cases (56.3%), incomplete occlusion in 6 (37.5%), and partial occlusion in 1 (6.3%). Intraprocedural complications included acute thrombosis in one case (6.3%) and re-rupture in another (6.3%). Both complications were managed appropriately with no sequela. Follow-up was performed in all patients for 3-24 months (mean, 7.7 months) after embolization. Complete occlusion was sustained in the 9 aneurysms with initial complete occlusion, progressive thrombosis to complete occlusion occurred in the 6 aneurysms with initial near-complete occlusion, and one aneurysm resulted in progressive thrombosis to complete occlusion after initial partial occlusion. No migration of stents or coils occurred at follow-up as compared with their positions immediately after embolization. At follow-up, all patients had recovered with no sequela.
CONCLUSION
The stent-assisted coil-jailing technique can be an efficient approach for tiny intracranial aneurysms, even though no definite conclusion regarding its safety can be drawn from the current data.
MeSH Terms
Figure
-

Fig. 1 58-year-old woman (patient 2) had sudden headache, nausea and vomiting for 18 hours. A. Tiny left posterior communicating artery aneurysm was shown. B. 1.5 mm × 3 cm coil was inserted into the aneurysm's sac and coil tail was constrained between stent and wall of internal carotid artery to increase coil stability. C. Deployed coil and its tail form shape of comma (arrow). D. Follow-up six months later revealed complete occlusion of aneurysm. Arrows indicate markers on distal and proximal ends of stent.

Fig. 2 46-year-old man (patient 1) who had subarachnoid hemorrhage was referred to our hospital for embolization of ruptured tiny aneurysm. 46-year-old man (patient 1) had tiny ruptured aneurysm at right ophthalmic artery segment of internal carotid artery (A). B. Aneurysm was treated with stent-assisted coiling technique. Small 1.5 mm × 2 cm coil was inserted into aneurysm's sac, and coil tail was compressed against wall of internal carotid artery by stent. Arrow indicates coil and constrained coil tail forming shape of comma. C. After stent was deployed, thrombi formed (small arrows) and 3000 IU heparin was infused together with 20 U urokinase. Bigger arrow indicates that anterior cerebral artery did not display very well because of thrombi. D. Fifteen minutes later, thrombi disappeared and patient was discharged with no sequela. Anterior cerebral artery was well displayed after thrombolysis (big arrow).
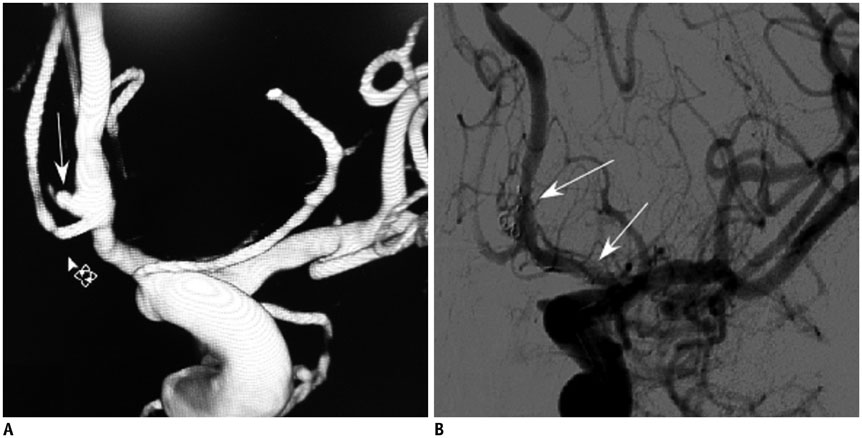
Fig. 3 57-year-old woman had sudden headache and nausea (patient 8). A. 57-year-old woman had tiny ruptured anterior communicating artery aneurysm (patient 8). B. Aneurysm was treated with stent-assisted coiling technique. Small 1.5 mm × 3 cm coil was inserted into aneurysm's sac and coil tail was compressed between stent (arrows) and vessel wall.
Cited by 1 articles
-
Outcomes of Stent-assisted Coil Embolization of Wide-necked Intracranial Aneurysms Using the Solitaire™ AB Neurovascular Remodeling Device
Hae Woong Jeong, Won-Bae Seung
J Cerebrovasc Endovasc Neurosurg. 2015;17(4):301-312. doi: 10.7461/jcen.2015.17.4.301.
Reference
-
1. Molyneux AJ, Kerr RS, Birks J, Ramzi N, Yarnold J, Sneade M, et al. Risk of recurrent subarachnoid haemorrhage, death, or dependence and standardised mortality ratios after clipping or coiling of an intracranial aneurysm in the International Subarachnoid Aneurysm Trial (ISAT): long-term follow-up. Lancet Neurol. 2009; 8:427–433.2. Brinjikji W, Lanzino G, Cloft HJ, Rabinstein A, Kallmes DF. Endovascular treatment of very small (3 mm or smaller) intracranial aneurysms: report of a consecutive series and a meta-analysis. Stroke. 2010; 41:116–121.3. Doerfler A, Wanke I, Egelhof T, Dietrich U, Asgari S, Stolke D, et al. Aneurysmal rupture during embolization with Guglielmi detachable coils: causes, management, and outcome. AJNR Am J Neuroradiol. 2001; 22:1825–1832.4. van Rooij WJ, Keeren GJ, Peluso JP, Sluzewski M. Clinical and angiographic results of coiling of 196 very small (< or = 3 mm) intracranial aneurysms. AJNR Am J Neuroradiol. 2009; 30:835–883.5. Yang MS, Wong HF, Yang TH, Chen YL, Chan SW, Lee HJ, et al. Alternative option in the treatment of very small ruptured intracranial aneurysms. Surg Neurol. 2009; 72:Suppl 2. S41–S46.6. Nussbaum ES, Erickson DL. The fate of intracranial microaneurysms treated with bipolar electrocoagulation and parent vessel reinforcement. Neurosurgery. 1999; 45:1172–1174. discussion 1174-1175.7. Wiebers DO, Whisnant JP, Huston J 3rd, Meissner I, Brown RD Jr, Piepgras DG, et al. Unruptured intracranial aneurysms: natural history, clinical outcome, and risks of surgical and endovascular treatment. Lancet. 2003; 362:103–110.8. Gupta V, Chugh M, Jha AN, Walia BS, Vaishya S. Coil embolization of very small (2 mm or smaller) berry aneurysms: feasibility and technical issues. AJNR Am J Neuroradiol. 2009; 30:308–314.9. Jeong YG, Jung YT, Kim MS, Eun CK, Jang SH. Size and location of ruptured intracranial aneurysms. J Korean Neurosurg Soc. 2009; 45:11–15.10. Cho CS. Coil Migration under Stent-Assisted Embolization. A Case Report. Interv Neuroradiol. 2006; 12:65–66.11. Gao BL, Li MH, Wang YL, Fang C. Delayed coil migration from a small wide-necked aneurysm after stent-assisted embolization: case report and literature review. Neuroradiology. 2006; 48:333–337.12. Nguyen TN, Raymond J, Guilbert F, Roy D, Bérubé MD, Mahmoud M, et al. Association of endovascular therapy of very small ruptured aneurysms with higher rates of procedure-related rupture. J Neurosurg. 2008; 108:1088–1092.13. Proust F, Debono B, Hannequin D, Gerardin E, Clavier E, Langlois O, et al. Treatment of anterior communicating artery aneurysms: complementary aspects of microsurgical and endovascular procedures. J Neurosurg. 2003; 99:3–14.14. Sluzewski M, Bosch JA, van Rooij WJ, Nijssen PC, Wijnalda D. Rupture of intracranial aneurysms during treatment with Guglielmi detachable coils: incidence, outcome, and risk factors. J Neurosurg. 2001; 94:238–240.15. Lim YC, Kim BM, Shin YS, Kim SY, Chung J. Structural limitations of currently available microcatheters and coils for endovascular coiling of very small aneurysms. Neuroradiology. 2008; 50:423–427.16. Bruening R, Mueller-Schunk S, Morhard D, Seelos KC, Brueckmann H, Schmid-Elsaesser R, et al. Intraprocedural thrombus formation during coil placement in ruptured intracranial aneurysms: treatment with systemic application of the glycoprotein IIb/IIIa antagonist tirofiban. AJNR Am J Neuroradiol. 2006; 27:1326–1331.17. Gralla J, Rennie AT, Corkill RA, Lalloo ST, Molyneux A, Byrne JV, et al. Abciximab for thrombolysis during intracranial aneurysm coiling. Neuroradiology. 2008; 50:1041–1047.18. Kang HS, Kwon BJ, Roh HG, Yoon SW, Chang HW, Kim JE, et al. Intra-arterial tirofiban infusion for thromboembolism during endovascular treatment of intracranial aneurysms. Neurosurgery. 2008; 63:230–237. discussion 237-238.19. Park JH, Kim JE, Sheen SH, Jung CK, Kwon BJ, Kwon OK, et al. Intraarterial abciximab for treatment of thromboembolism during coil embolization of intracranial aneurysms: outcome and fatal hemorrhagic complications. J Neurosurg. 2008; 108:450–457.20. Thornton J, Debrun GM, Aletich VA, Bashir Q, Charbel FT, Ausman J. Follow-up angiography of intracranial aneurysms treated with endovascular placement of Guglielmi detachable coils. Neurosurgery. 2002; 50:239–249. discussion 249-250.21. Raymond J, Guilbert F, Weill A, Georganos SA, Juravsky L, Lambert A, et al. Long-term angiographic recurrences after selective endovascular treatment of aneurysms with detachable coils. Stroke. 2003; 34:1398–1403.
- Full Text Links
-
- Actions
-
Cited
- CITED
-
- Close
- Share
-
- Similar articles
-
- The Stent-Assisted Coil-Jailing Technique Facilitates Efficient Embolization of Tiny Cerebral Aneurysms
- Preliminary Results of Y-Stent-Assisted Coil Embolization of Wide-Necked Intracranial Aneurysms: 8 Consecutive Patients
- Stent-assisted Coil Embolization of Cerebral Aneurysms: Review Article
- A Complicated Case of Endovascular Stent Assisted Coil Embolization of an Aneurysm
- Subarachnoid Hemorrhage from a Dissecting Aneurysm of the Posterior Cerebral Artery in a Child : Rebleeding after Stent-Assisted Coiling Followed by Stent-Within-Stent Technique
