US Features of Transient Small Bowel Intussusception in Pediatric Patients
- Affiliations
-
- 1Department of Radiology and Center for Imaging Science, Samsung Medical Center, Sungkyunkwan University School of Medicine, Korea. jhkate.kim@samsung.com
- KMID: 1118823
- DOI: http://doi.org/10.3348/kjr.2004.5.3.178
Abstract
OBJECTIVE
To describe the sonographic (US) and clinical features of spontaneously reduced small bowel intussusception, and to discuss the management options for small bowel intussusception based on US findings with clinical correlation. MATERIALS AND METHODS: During a five years of period, 34 small bowel intussusceptions were diagnosed on US in 32 infants and children. The clinical presentations and imaging findings of the patients were reviewed. RESULTS: The clinical presentations included abdominal pain or irritability (n = 25), vomiting (n = 5), diarrhea (n = 3), bloody stool (n = 1), and abdominal distension (n = 1), in combination or alone. US showed multi-layered round masses of small (mean, 1.5+/-0.3 cm) diameters and with thin (mean, 3.5+/-1 mm) outer rims along the course of the small bowel. The mean length was 1.8+/-0.5 cm and peristalsis was seen on the video records. There were no visible lead points. The vascular flow signal appeared on color Doppler images in all 21 patients examined. Spontaneous reduction was confirmed by combinations of US (n = 28), small bowel series (n = 6), CT scan (n = 3), and surgical exploration (n = 2). All patients discharged with improved condition. CONCLUSION: Typical US findings of the transient small bowel intussusception included 1) small size without wall swelling, 2) short segment, 3) preserved wall motion, and 4) absence of the lead point. Conservative management with US monitoring rather than an immediate operation is recommended for those patient with typical transient small bowel intussusceptions. Atypical US findings or clinical deterioration of the patient with persistent intussusception warrant surgical exploration.
MeSH Terms
Figure
-

Fig. 1 Typical benign small bowel intussusception in a 9-year-old boy with abdominal pain after chemotherapy for mediastinal lymphoma. Transverse (A) and longitudinal (B) US scans show crescent-in-doughnut (A) and sandwich sign (B). The diameter of the doughnut is 1.9 cm and the length of the lesion is 2.5 cm.
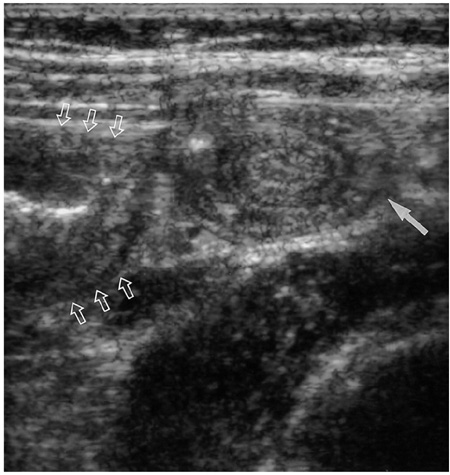
Fig. 2 Small bowel intussusception associated with ileocolic intussusception in a 3-year-old girl. Immediate post-enema US reveals a multi-layered mass (solid arrow) suggesting small bowel intussusception, adjacent to the swollen reduced terminal ileum (open arrows). The small bowel intussusception spontaneously reduced during US examination and her abdominal pain subsided.

Fig. 3 Idiopathic postoperative small bowel intussusception in a 3 month-old-girl who underwent surgical reduction of the ileocolic intussusception. A. Plain radiography obtained 4 days after laparotomy shows the distended bowel and mass-like shadow at the right upper quadrant. B. Recurrent intussusception was suspected and US scan revealed a small (diameter, 1.3 cm) small bowel intussusception in the left abdomen. There was not any ieocolic intussusception corresponding to the right upper abdominal mass seen on A. Repeated US 5 hours later demonstrated the disappearance of the small bowel intussusception and follow-up radiography (C) shows improved bowel distension. The patient recovered uneventfully thereafter and was discharged.

Fig. 4 Fluid retention between the walls of invaginated bowel in a 2-year-old boy who presented with intermittent irritable crying. Longitudinal US scan shows the short-segmental small bowel intussusception with entrapped fluid (arrows) between the intussuscepient and intussusceptum. Repeated US 1 hour later did not demonstrate the small bowel intussusception any more and the patient discharged with an improved state.
Cited by 1 articles
-
Small Bowel Intussusception in Children: Spontaneous Resolution vs. Surgical Intervention
Mi Ran Park, Mi Sun Lim, Jeong Kee Seo, Jae Sung Ko, Ju Young Chang, Hye Ran Yang, Yoon Joung Lim, Woo Sun Kim
Korean J Pediatr Gastroenterol Nutr. 2010;13(2):128-133. doi: 10.5223/kjpgn.2010.13.2.128.
Reference
-
1. del-Pozo G, Albillos JC, Tejedor D, et al. Intussusception in children: current concepts in diagnosis and enema reduction. RadioGraphics. 1999. 19:299–319.2. Stone DN, Kangarloo H, Graviss ER, Danis RK, Silberstein MJ. Jejunal intussusception in children. Pediatr Radiol. 1980. 9:65–68.3. Hughes UM, Connolly BL, Chait PG, Muraca S. Further report of small-bowel intussusceptions related to gastrojejunostomy tubes. Pediatr Radiol. 2000. 30:614–617.4. Jequier S, Argyropoulou M, Bugmann P. Ultrasonography of jejunal intussusception in children. Can Assoc Radiol J. 1995. 46:285–290.5. Carnevale E, Graziani M, Fasanelli S. Post-operative ileo-ileal intussusception: sonographic approach. Pediatr Radiol. 1994. 24:161–163.6. Shanbhogue RL, Hussain SM, Meradji M, Robben SG, Vernooij JE, Molenaar JC. Ultrasonography is accurate enough for the diagnosis of intussusception. J Pediatr Surg. 1994. 29:324–327.7. Ko SF, Lee TY, Ng SH, et al. Small bowel intussusception in symptomatic pediatric patients: experiences with 19 surgically proven cases. World J Surg. 2002. 26:438–443. Epub 2002 Jan 21.8. Tiao MM, Wan YL, Ng SH, et al. Sonographic features of small-bowel intussusception in pediatric patients. Acad Emerg Med. 2001. 8:368–373.9. Kornecki A, Daneman A, Navarro O, Connolly B, Manson D, Alton DJ. Spontaneous reduction of intussusception: clinical spectrum, management and outcome. Pediatr Radiol. 2000. 30:58–63.10. Strouse PJ, DiPietro MA, Saez F. Transient small-bowel intussusception in children on CT. Pediatr Radiol. 2003. 33:316–320. Epub 2003 Feb 26.11. Doi O, Aoyama K, Hutson JM. Twenty-one cases of small bowel intussusception: the pathophysiology of idiopathic intussusception and the concept of benign small bowel intussusception. Pediatr Surg Int. 2004. 02. 10. (Epub ahead of print).12. Lvoff N, Breiman RS, Coakley FV, Lu Y, Warren RS. Distinguishing features of self-limiting adult small-bowel intussusception identified at CT. Radiology. 2003. 227:68–72.13. Britton I, Wilkinson AG. Ultrasound features of intussusception predicting outcome of air enema. Pediatr Radiol. 1999. 29:705–710.14. Lim HK, Bae SH, Lee KH, Seo GS, Yoon GS. Assessment of reducibility of ileocolic intussusception in children: usefulness of color Doppler sonography. Radiology. 1994. 191:781–785.15. Lagalla R, Caruso G, Novara V, Derchi LE, Cardinale AE. Color Doppler ultrasonography in pediatric intussusception. J Ultrasound Med. 1994. 13:171–174.16. Luckey P, Kemper J, Engelbrecht V, Modder U. Idiopathic ileoileal intussusception in an adult with spontaneous reduction during enteroclysis: a case report. Abdom Imaging. 2000. 25:48–50.17. Hanquinet S, Anooshiravani M, Vunda A, Le Coultre C, Bugmann P. Reliability of color Doppler and power Doppler sonography in the evaluation of intussuscepted bowel viability. Pediatr Surg Int. 1998. 13:360–362.18. Swischuk LE, John SD, Swischuk PN. Spontaneous reduction of intussusception: verification with US. Radiology. 1994. 192:269–271.19. Mapagu C, Lam A, Martin HC, Fitzgerald DA. Intermittent intussusception. J Paediatr Child Health. 2003. 39:147–148.20. Sonmez K, Turkyilmaz Z, Demirogullari B, et al. Conservative treatment for small intestinal intussusception associated with Henoch-Schonlein's purpura. Surg Today. 2002. 32:1031–1034.
- Full Text Links
-
- Actions
-
Cited
- CITED
-
- Close
- Share
-
- Similar articles
-
- A Case of Recurrent Transient Small Bowel Intussusception
- Clinical features of transient small bowel intussusception in children
- US Features of Transient Small Bowel Intussusception in Pediatric Patients
- A Case of Transient Small Intestinal Intussusceptions in an Adult
- A Clinical Observation on Children with Transient Small Bowel Intussusception
