Toxic Inhalational Injury-Associated Interstitial Lung Disease in Children
- Affiliations
-
- 1Department of Pediatrics, Asan Medical Center Children's Hospital, Asan Medical Center, University of Ulsan College of Medicine, Seoul, Korea. sjhong@amc.seoul.kr
- 2Childhood Asthma Atopy Center, Asan Medical Center Children's Hospital, Asan Medical Center, University of Ulsan College of Medicine, Seoul, Korea.
- 3Research Center for Standardization of Allergic Diseases, Asan Medical Center Children's Hospital, Asan Medical Center, University of Ulsan College of Medicine, Seoul, Korea.
- 4Department of Pediatrics, Korea Cancer Center Hospital, Seoul, Korea.
- 5Department of Pediatrics, Kosin University College of Medicine, Busan, Korea.
- 6Department of Pediatrics, Seoul National University Bundang Hospital, Seongnam, Korea.
- 7Department of Pediatrics, Inje University Haeundae Paik Hospital, Buasn, Korea.
- 8Department of Radiology, Asan Medical Center, University of Ulsan College of Medicine, Seoul, Korea.
- 9Department of Pathology, Asan Medical Center, University of Ulsan College of Medicine, Seoul, Korea.
- KMID: 2158041
- DOI: http://doi.org/10.3346/jkms.2013.28.6.915
Abstract
- Interstitial lung disease in children (chILD) is a group of disorders characterized by lung inflammation and interstitial fibrosis. In the past recent years, we noted an outbreak of child in Korea, which is possibly associated with inhalation toxicity. Here, we report a series of cases involving toxic inhalational injury-associated chILD with bronchiolitis obliterans pattern in Korean children. This study included 16 pediatric patients confirmed by lung biopsy and chest computed tomography, between February 2006 and May 2011 at Asan Medical Center Children's Hospital. The most common presenting symptoms were cough and dyspnea. The median age at presentation was 26 months (range: 12-47 months), with high mortality (44%). Histopathological analysis showed bronchiolar destruction and centrilobular distribution of alveolar destruction by inflammatory and fibroproliferative process with subpleural sparing. Chest computed tomography showed ground-glass opacities and consolidation in the early phase and diffuse centrilobular nodular opacity in the late phase. Air leak with severe respiratory difficulty was associated with poor prognosis. Although respiratory chemicals such as humidifier disinfectants were strongly considered as a cause of this disease, further studies are needed to understand the etiology and pathophysiology of the disease to improve the prognosis and allow early diagnosis and treatment.
MeSH Terms
-
APACHE
Bronchi/pathology
Child, Preschool
Cough/etiology
Cyclophosphamide/therapeutic use
Disinfectants/*toxicity
Dyspnea/etiology
Enzyme Inhibitors/therapeutic use
Humans
Hydroxychloroquine/therapeutic use
Immunoglobulins/therapeutic use
Infant
Inhalation
Lung Diseases, Interstitial/chemically induced/drug therapy/*pathology
Prognosis
Retrospective Studies
Steroids/therapeutic use
Tomography, X-Ray Computed
Disinfectants
Enzyme Inhibitors
Immunoglobulins
Steroids
Hydroxychloroquine
Cyclophosphamide
Figure
-

Fig. 1 Lung histology in two patients with toxic inhalational lung injury associated with interstitial lung disease in children. (A) Air spaces are diffusely filled with edema fluid. Alveolar septa are focally infiltrated by lymphocytes (H&E, original magnification ×200). (B) A few bronchioles are disrupted and infiltrated by lymphocytes (arrows) (H&E, Original magnification ×400). (C) Alveolar septa are thickened by inflammatory infiltration. Hyaline membranes are deposited air-side of alveolar septa (arrow). Histiocytes with occasional foamy change fill alveolar spaces (H&E, original magnification ×400). (D) Low magnification of this example shows prominent centrilobular distribution of interstitial thickening and fibrosis (H&E, Original magnification ×40). (E) Bronchioles are destructed by inflammatory cells (arrow) and fibroblastic proliferation (asterisk) and epithelial cells are denuded. Peribronchiolar interstitial septa are severely thickened with infiltration of chronic inflammatory cells, fibroblasts and foamy histiocytes (left half) (H&E, Original magnification ×200). (F) Fibroblastic proliferation in pale myxoid stroma obliterates the bronchiolar space (asterisk). Collapsed alveolar spaces are lined by activated pneumocytes and filled with collection of foamy histiocytes (arrow) (H&E, original magnification ×200).
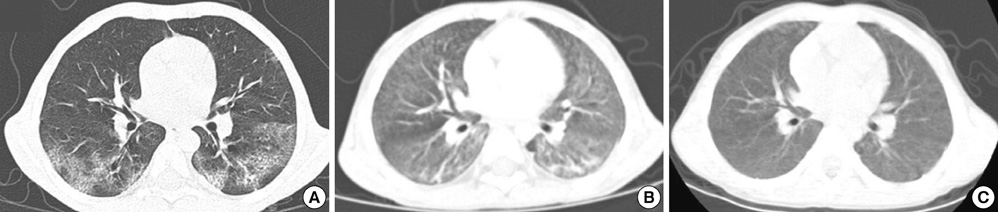
Fig. 2 Radiologic findings in a 41-month-old boy with toxic inhalational lung injury associated interstitial lung disease. (A) A high resolution computed tomography scan performed 2 weeks after symptom onset demonstrates focal patchy consolidation and ground-glass opacity in both lower lobes with subpleural sparing. (B) Chest CT scan of the patient 6 weeks after symptom onset shows progression of diffuse centrilobular nodules with ground-glass opacity, suggesting peribronchiolar fibrosis in both lungs. (C) One-year follow-up chest CT scan shows decreased density, but residual diffuse centrilobular ground-glass opacity involving both lungs.
Cited by 7 articles
-
Comparison of Long Term Follow-up Chest CT Imaging in Adult and Pediatric Patients with Humidifier Disinfectant-related Lung Injury
Soyeoun Lim, Jong Han Leem, Young-Seoub Hong, Jungwon Kim, Soyoung Park, Joon-Sung Joh, Woon-Jung Kwon, Yangho Kim
J Korean Med Sci. 2020;35(45):e377. doi: 10.3346/jkms.2020.35.e377.Two Cases of Chloromethylisothiazolinone and Methylisothiazolinone-associated Toxic Lung Injury
Eun Lee, Seung Kook Son, Jisun Yoon, Hyun-Ju Cho, Song-I Yang, Sungsu Jung, Kyung-Hyun Do, Young Ah Cho, So-Yeon Lee, Dong-Uk Park, Soo-Jong Hong
J Korean Med Sci. 2018;33(16):. doi: 10.3346/jkms.2018.33.e119.The Pathological Findings of Chloromethylisothiazolinone and Methylisothiazolinone-associated Lung Injury
So-Yeon Lee, Dong-Uk Park, Kyung-Hyun Do, Se-Jin Jang, Soo-Jong Hong
J Korean Med Sci. 2019;34(14):. doi: 10.3346/jkms.2019.34.e102.Characteristics of pediatric noniatrogenic pneumomediasinum
Narae Lee, Seung Kook Son, Hyung Young Kim, Hye-Young Kim, Hee Ju Park
Allergy Asthma Respir Dis. 2015;3(2):145-150. doi: 10.4168/aard.2015.3.2.145.Problems with diagnostic criteria for humidifier disinfectant lung injury (HDLI): two cases of radiologically improved HDLI
Min-Woo Nam, So-Young Park, Byung-Seong Suh, Soo-Youn Ham, Kyung-Hun Son, Hyunil Kim, Hyeong-Cheol Kim
Ann Occup Environ Med. 2020;32:e1. doi: 10.35371/aoem.2020.32.e1.Problems with diagnostic criteria for humidifier disinfectant lung injury (HDLI): two cases of radiologically improved HDLI
Min-Woo Nam, So-Young Park, Byung-Seong Suh, Soo-Youn Ham, Kyung-Hun Son, Hyunil Kim, Hyeong-Cheol Kim
Ann Occup Environ Med. 2020;32(1):. doi: 10.35371/aoem.2020.32.e1.Health Effects Associated With Humidifier Disinfectant Use: A Systematic Review for Exploration
Ji-Hun Song, Joonho Ahn, Min Young Park, Jaeyoung Park, Yu Min Lee, Jun-Pyo Myong, Jung-Wan Koo, Jongin Lee
J Korean Med Sci. 2022;37(33):e257. doi: 10.3346/jkms.2022.37.e257.
Reference
-
1. Deschildre A, Leclerc F, Hue V, Martinot A, Flurin V, Fourier C, Devisme L, Ramon P, Wallaert B. Treatment with intermittent high dosage corticotherapy in chronic interstitial pneumonia in an infant: a case report. Rev Mal Respir. 1994. 11:509–512.2. Clement A, Eber E. Interstitial lung diseases in infants and children. Eur Respir J. 2008. 31:658–666.3. Cheon CK, Jin HS, Kang EK, Kim HB, Kim BJ, Yu J, Park SJ, Hong SJ, Park JD. Epidemic acute interstitial pneumonia in children occurred during the early 2006s. Korean J Pediatr. 2008. 51:383–390.4. Kim BJ, Kim HA, Song YH, Yu J, Kim S, Park SJ, Kim KW, Kim KE, Kim DS, Park JD, et al. Nationwide surveillance of acute interstitial pneumonia in Korea. Korean J Pediatr. 2009. 52:324–329.5. Küpeli E, Karnak D, Kayacan O, Beder S. Clues for the differential diagnosis of hypersensitivity pneumonitis as an expectant variant of diffuse parenchymal lung disease. Postgrad Med J. 2004. 80:339–345.6. Yang HJ, Kim HJ, Yu JH, Lee E, Jung YH, Kim HY, Seo JH, Kwon GY, Park JH, Gwack J, et al. Inhalation toxicity of humidifier disinfectants as a risk factor of children's interstitial lung disease in Korea: a case-control study. PLoS One. 2013. doi: 10.1371/journal.pone.0064430.7. Kim JY, Kim HH, Cho KH. Acute cardiovascular toxicity of sterilizers, PHMG, and PGH: severe inflammation in human cells and heart failure in zebrafish. Cardiovasc Toxicol. 2013. 13:148–160.8. Langston C, Fan LL. Diffuse interstitial lung disease in infants. Pediatr Pulmonol. 2001. Suppl 23. 74–76.9. Lee E, Seo JH, Kim HY, Yu J, Song JW, Park YS, Jang SJ, Do KH, Kwon J, Park SW, et al. Two series of familial cases with unclassified interstitial pneumonia with fibrosis. Allergy Asthma Immunol Res. 2012. 4:240–244.10. Yousem SA, Dacic S. Idiopathic bronchiolocentric interstitial pneumonia. Mod Pathol. 2002. 15:1148–1153.11. Kwon SY, Kim JM, Sohn MH, Kim DS, Kim MJ, Cho SH. Acute interstitial pneumonia in siblings: a case report. J Korean Med Sci. 2008. 23:529–532.12. Deutsch GH, Young LR, Deterding RR, Fan LL, Dell SD, Bean JA, Brody AS, Nogee LM, Trapnell BC, Langston C, et al. Diffuse lung disease in young children: application of a novel classification scheme. Am J Respir Crit Care Med. 2007. 176:1120–1128.13. Langston C, Dishop MK. Diffuse lung disease in infancy: a proposed classification applied to 259 diagnostic biopsies. Pediatr Dev Pathol. 2009. 12:421–437.14. Dishop MK. Paediatric interstitial lung disease: classification and definitions. Paediatr Respir Rev. 2011. 12:230–237.15. Korea Centers for Disease Control and Prevention. accessed on 30 January 2013. Available at http://www.cdc.go.kr/CDC/intro/CdcKrIntro0201.jsp?menuIds=HOME001-MNU0005-MNU0011&cid=9437.16. Ministry of Health & Welfare. accessed on 30 January 2013. Available at http://www.mw.go.kr/front/mw_sch/index.jsp.17. Miller K, Chang A. Acute inhalation injury. Emerg Med Clin North Am. 2003. 21:533–557.18. Amin RS, Wert SE, Baughman RP, Tomashefski JF Jr, Nogee LM, Brody AS, Hull WM, Whitsett JA. Surfactant protein deficiency in familial interstitial lung disease. J Pediatr. 2001. 139:85–92.19. Nogee LM. Genetics of pediatric interstitial lung disease. Curr Opin Pediatr. 2006. 18:287–292.20. Silva CI, Churg A, Müller NL. Hypersensitivity pneumonitis: spectrum of high-resolution CT and pathologic findings. AJR Am J Roentgenol. 2007. 188:334–344.21. King TE Jr. Clinical advances in the diagnosis and therapy of the interstitial lung diseases. Am J Respir Crit Care Med. 2005. 172:268–279.22. Fan LL, Langston C. Pediatric interstitial lung disease: children are not small adults. Am J Respir Crit Care Med. 2002. 165:1466–1467.23. Hewitt CJ, Hull D, Keeling JW. Fibrosing alveolitis in infancy and children. Arch Dis Child. 1977. 52:22–37.24. Olson J, Colby TV, Elliott CG. Hamman-Rich syndrome revisited. Mayo Clin Proc. 1990. 65:1538–1548.25. Quefatieh A, Stone CH, DiGiovine B, Toews GB, Hyzy RC. Low hospital mortality in patients with acute interstitial pneumonia. Chest. 2003. 124:554–559.26. Suh GY, Kang EH, Chung MP, Lee KS, Han J, Kitaichi M, Kwon OJ. Early intervention can improve clinical outcome of acute interstitial pneumonia. Chest. 2006. 129:753–761.
- Full Text Links
-
- Actions
-
Cited
- CITED
-
- Close
- Share
-
- Similar articles
-
- Toxic Inhalational Injury-Associated Interstitial Lung Disease in Children
- The past, present, and future of humidifier disinfectant-associated interstitial lung diseases in children
- Idiopathic interstitial pneumonias: clinical findings, pathogenesis, pathology and radiologic findings
- Idiopathic Interstitial Pneumonias: Radiologic Findings
- A Case of Interstitial Pneumonitis with Acute Live Injury Caused by Herbal Medicine Made from Golden Thread
