Gastric Bleeding Arisen in a Patient with Situs Inversus Totalis and Large Accessory Spleen
- Affiliations
-
- 1Department of Surgery, Cheongju St. Mary's Hospital, Cheongju, Korea. gsurgeonl@naver.com
- 2Department of Internal Medicine, Cheongju St. Mary's Hospital, Cheongju, Korea.
- 3Department of Pathology, Cheongju St. Mary's Hospital, Cheongju, Korea.
- 4Center for Health Promotion, Samsung Medical Center, Seoul, Korea.
- KMID: 1750740
- DOI: http://doi.org/10.4174/jkss.2010.78.4.258
Abstract
- Situs inversus totalis is a rare congenital disorder, which is total transposition of thoracic and abdominal organs. Its incidence is 1 in 10,000~50,000 live births. This might be associated with multiple abnormalities such as accessory spleen, asplenia, intestinal malrotation and so on. For this reason, in cases of operation in patients with situs inversus totalis, we need to scrutinize the presence of accompanied anomalies. Moreover, if Dieulafoy gastric bleeding has occurred, vascular anomalies can be accompanied. This 31-year-old male patient with situs inverses totalis was admitted to our hospital for management of UGI (upper gastrointestinal) bleeding. Gastroendoscopy revealed Dieulafoy disease in the upper body of the stomach as the cause of UGI bleeding. Several attempts with endovascular embolization and hemoclips were applied but failed. We performed a suture & ligation of the Dieulafoy lesion as well as total resection of accessory spleen with devascularization of prominently developed vessels around the upper stomach. We report this case with a review of the literature.
MeSH Terms
Figure
-

Fig. 1 Chest X-ray; Situs inversus totalis is suggested. Severe diffuse fatty liver with hepatomegaly is demonstrated.
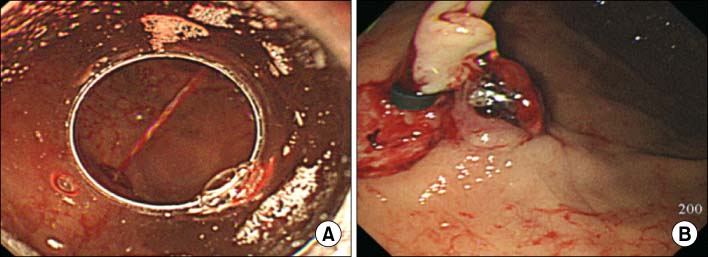
Fig. 2 (A) Gastroscopy shows spurting blood from upper body of the stomach. (B) Gastroscopy shows hemoclip & fibrin glue on the exposed vessel.
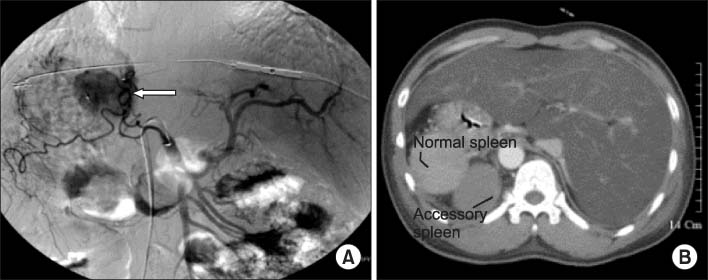
Fig. 3 (A) SMA (sup. Mesenteric artery) angiogram shows common hepatic, splenic and gastroduodenal arteries originated from SMA as well as round hypervascular mass at the medial aspect of upper body of the stomach. (B) Abdominal CT. Non-enhancing ovoid mass in the site of right adrenal gland at posterior surface of normal spleen is seen.
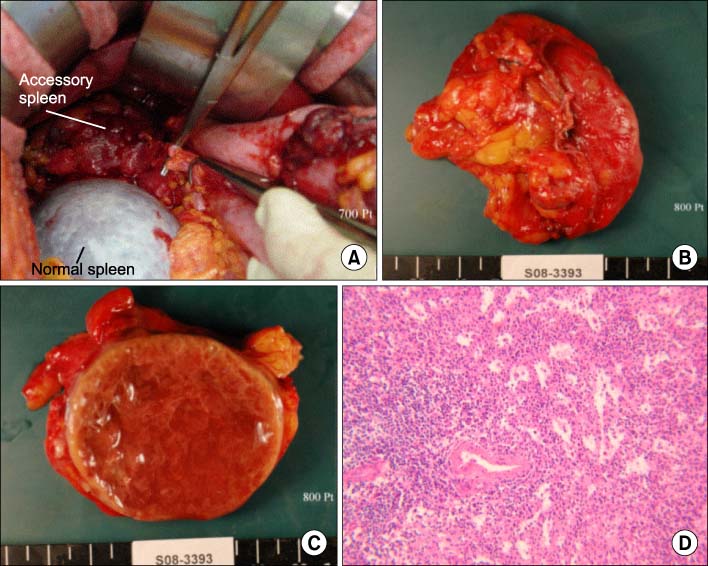
Fig. 4 (A) Operative field shows clamping of presumptive feeding vessel of large mass (accessory spleen) on the medial side of the stomach adjacent to normal spleen. (B) The specimen consists of an oval shaped, well-circumscribed and solid mass. (C) The cut surface of accessory spleen is totally necrotic because of embolization of hypervascular mass for control of gastric bleeding. (D) Accessory spleen shows infarctive necrosis and congestion (H&E, ×100).
Cited by 2 articles
-
Gastrostomy in a Patient with Situs Inversus Totalis
Hyung Ki Lee, Kwang Bum Cho, Eun Soo Kim, Kyung Sik Park
Clin Endosc. 2013;46(6):662-665. doi: 10.5946/ce.2013.46.6.662.Death due to Gastrointestinal Hemorrhage Associated with Dieulafoy's Lesion
Jaehong Park, Hongil Ha, Minjung Kim
Korean J Leg Med. 2014;38(3):113-115. doi: 10.7580/kjlm.2014.38.3.113.
Reference
-
1. Pavlidis TE, Psarras K, Triantafyllou A, Marakis GN, Sakantamis AK. Laparoscopic cholecystectomy for severe acute cholecystitis in a patient with situs inversus totalis and posterior cystic artery. Diagn Ther Endosc. 2008. 2008:465272.2. Rudowski WJ. Accessory spleens: clinical significance with particular reference to the recurrence of idiopathic thrombocytopenic purpura. World J Surg. 1985. 9:422–430.3. Fujiwara Y, Fukunaga Y, Higashino M, Tanimura S, Takemura M, Tanaka Y, et al. Laparoscopic hemicolectomy in a patient with situs inversus totalis. World J Gastroenterol. 2007. 13:5035–5037.4. Yi SQ, Tanaka S, Tanaka A, Shimokawa T, Ru F, Nakatani T. An extremely rare inversion of the preduodenal portal vein and common bile duct associated with multiple malformations. Report of an adult cadaver case with a brief review of the literature. Anat Embryol (Berl). 2004. 208:87–96.5. Marta MJ, Falcao LM, Saavedra JA, Ravara L. A case of complete situs inversus. Rev Port Cardiol. 2003. 22:91–104.6. Mumtaz R, Shaukat M, Ramirez FC. Outcomes of endoscopic treatment of gastroduodenal Dieulafoy's lesion with rubber band ligation and thermal/injection therapy. J Clin Gastroenterol. 2003. 36:310–314.7. Alshumrani G, Almuaikeel M. Angiographic findings and endovascular embolization in Dieulafoy disease: a case report and literature review. Diagn Interv Radiol. 2006. 12:151–154.8. Juler GL, Labitzke HG, Lamb R, Allen R. The pathogenesis of Dieulafoy's gastric erosion. Am J Gastroenterol. 1984. 79:195–200.9. Grace PA, O'Sullivan R, Adam AN, Williamson RC. Case report: vascular anomaly in Dieulafoy's disease. Clin Radiol. 1991. 44:201–202.
- Full Text Links
-
- Actions
-
Cited
- CITED
-
- Close
- Share
-
- Similar articles
-
- Gastric Bleeding Arisen in a Patient with Situs Inversus Totalis and Large Accessory Spleen
- A case of Congenital Asplenia Associated Dextrocardia with Situs Inversus Totalis
- Radical Subtotal Gastrectomy in Early Gastric Cancer Patient with Situs Inversus Totalis
- Single Port Laparoscopic Cholecystectomy in a Patient with Situs Inversus Totalis: A Case Report
- Neonatal Duodenal Obstruction Associated with Situs Inversus Totalis: A Case Report
