Intravitreal Ranibizumab Therapy for Neovascular Age-Related Macular Degeneration with a Predominantly Hemorrhagic Lesion
- Affiliations
-
- 1Department of Ophthalmology, Kang Dong Sacred Heart Hospital, Hallym University College of Medicine, Seoul, Korea. sungpyo@hanafos.com
- KMID: 2214709
- DOI: http://doi.org/10.3341/jkos.2011.52.7.838
Abstract
- PURPOSE
To report the efficacy and safety of intravitreal ranibizumab monotherapy in patients with age-related macular degeneration with a predominantly hemorrhagic lesion.
METHODS
Nineteen eyes of 19 patients with submacular hemorrhage involving the fovea were treated with intravitreal ranibizumab (0.5 mg/0.05 ml) injections as needed. All patients completed at least 4 months of follow-up. Ophthalmologic examinations, fluorescence angiographic evaluations, optical coherence tomography (OCT) examination, and hemorrhage size were analyzed before the injections, and at 1,2,4,6, and 12 months follow-up.
RESULTS
The average VA and mean central retinal thickness (CRT) before ranibizumab treatment were 0.62 +/- 0.39 log MAR and 335.76 +/- 111.22 microm, respectively. Additionally, the VA and CRT four months after the initial injections were 0.54 +/- 0.43 log MAR and 241.42 +/- 107.55 microm, respectively. The mean size of the hemorrhage was significantly reduced from 2.87 +/- 2.44 DA (disk areas) at baseline to 0.9 +/- 1.28 DA at four month follow up.
CONCLUSIONS
Intravitreal injection of ranibizumab is an effective treatment option for patients with age-related macular degeneration with a predominantly hemorrhagic lesion.
MeSH Terms
Figure
-
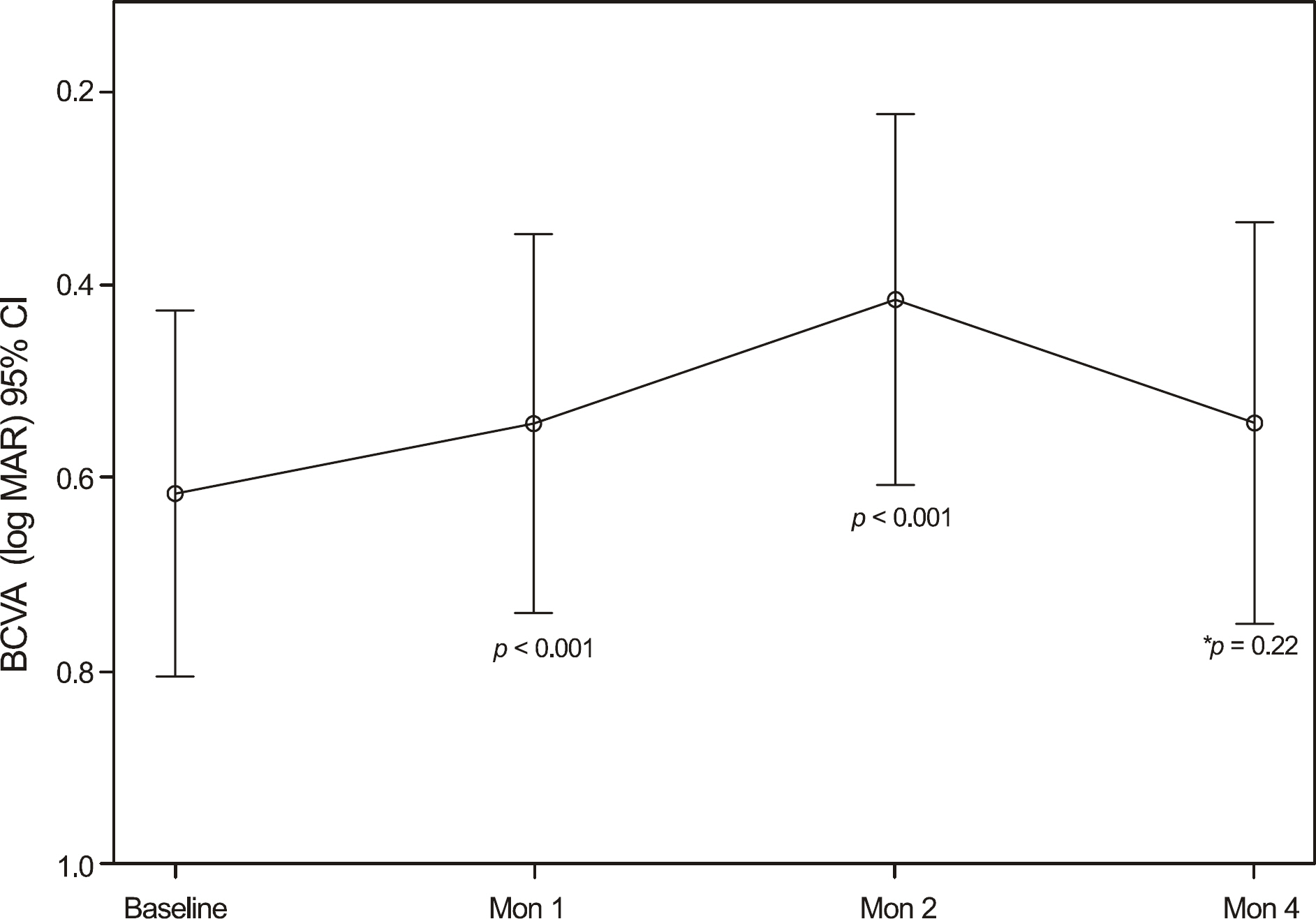
Figure 1. Changes in best corrected visual acuity (BCVA) after intravitreal ranibizumab injection. Best corrected visual acuity improved at 1 month from baseline, a difference that was statistically significant (p < 0.001), this level of BCVA was maintained throughout 2 months. * Not significant differences.

Figure 2. Changes in central macular thickness with OCT during follow-up after intravitreal ranibizumab injection. The foveal thickness improved after 1 month, the mean central macular thickness measurements decreased from 335.74 ± 111.22 μ m to 271.42 ± 76.9 μ m (p = 0.006) and this overall improvement continued throughout 4 month follow-up.

Figure 3. Correlation analysis between the decrease of central macular thickness and the improvement of best-corrected visual acuity (BCVA) four months after initial treatment (Pearson correlation, r = 0.45; p= 0.055).
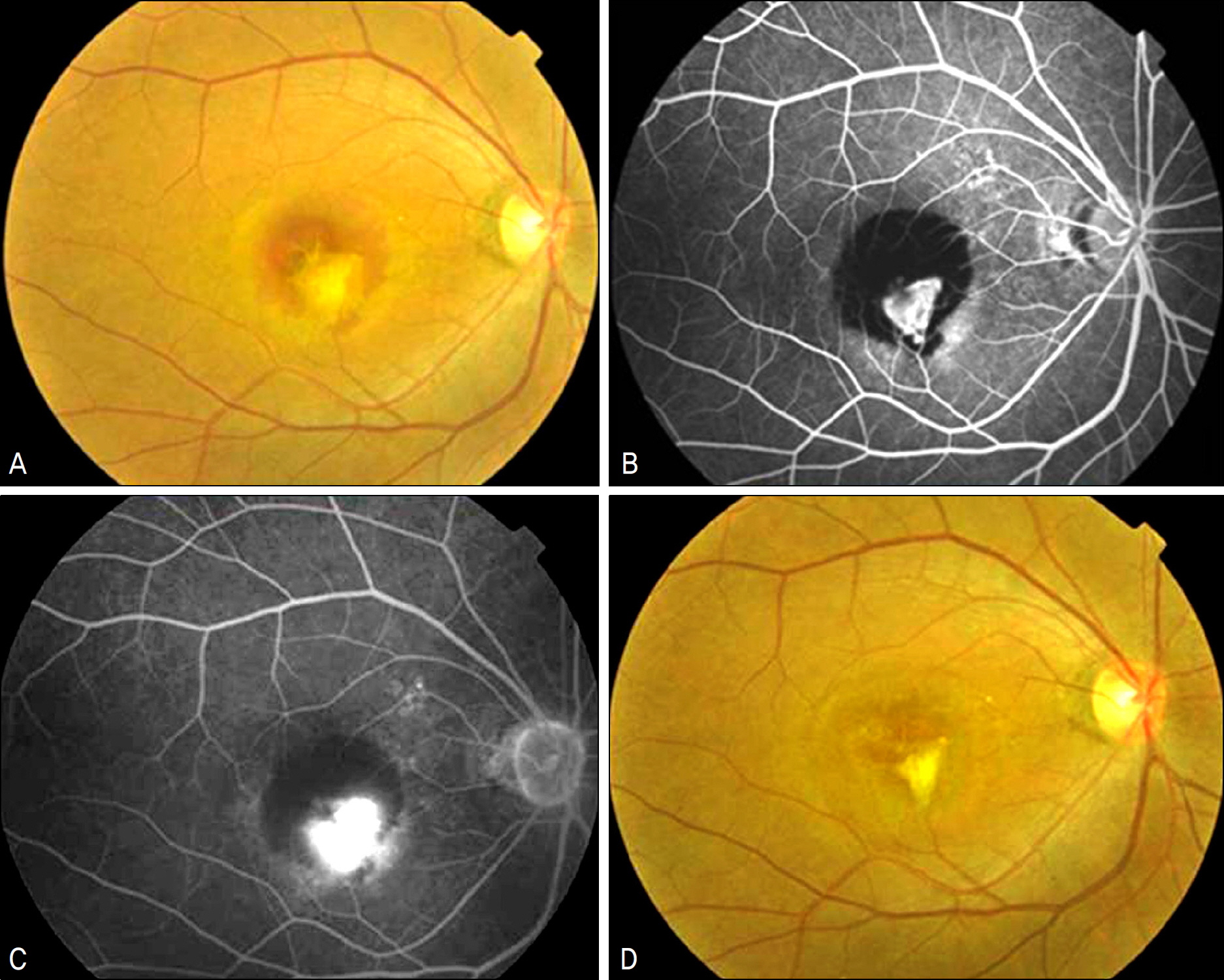
Figure 4. The fundus photographs (A, D), fluorescein angiographs (B, C) of patient 18. (A) Baseline fundus photograph showed submacular hemorrhage. (B, C) Early and late phase fluorescein angiography at baseline. Blocked fluorescence is seen around the hyperfluorescence. (D) Fundus photograph at 4 months after treatment showed resolution of hemorrhage.
Reference
-
References
1. Brown DM, Michels M, Kaiser PK, et al. Ranibizumab versus verteporfin photodynamic therapy for neovascular age-related macular degeneration: Two-year results of the ANCHOR study. Ophthalmology. 2009; 116:57–65.
Article2. Avery RL, Fekrat S, Hawkins BS, Bressler NM. Natural history of subfoveal subretinal hemorrhage in age-related macular degeneration. Retina. 1996; 16:183–9.
Article3. Bennett SR, Folk JC, Blodi CF, Klugman M. Factors prognostic of visual outcome in patients with subretinal hemorrhage. Am J Ophthalmol. 1990; 109:33–7.
Article4. Berrocal MH, Lewis ML, Flynn HW Jr. Variations in the clinical course of submacular hemorrhage. Am J Ophthalmol. 1996; 122:486–93.
Article5. Sanders D, Peyman GA, Fishman G, et al. The toxicity of intravitreal whole blood and hemoglobin. Albrecht Von Graefes Arch Klin Exp Ophthalmol. 1975; 197:255–67.
Article6. Toth CA, Morse LS, Hjelmeland LM, Landers MB 3rd. Fibrin di-rects early retinal damage after experimental subretinal hemorrhage. Arch Ophthalmol. 1991; 109:723–9.
Article7. Glatt H, Machemer R. Experimental subretinal hemorrhage in rabbits. Am J Ophthalmol. 1982; 94:762–73.
Article8. Hewitt AT, Adler R. The retinal pigment epithelium and interphotoreceptor matrix: structure and specialized functions. Ryan SJ, editor. Retina. St. Louise: CV Mosby;1994. 1:p. 58–71.9. Photodynamic therapy of subfoveal choroidal neovascularization in age-related macular degeneration with verteporfin: one-year results of 2 randomized clinical trials–TAP report. Treatment of age-related macular degeneration with photodynamic therapy (TAP) Study Group. Arch Ophthalmol. 1999; 117:1329–45.10. Rosenfeld PJ, Brown DM, Heier JS, et al. Ranibizumab for neovascular age-related macular degeneration. N Engl J Med. 2006; 355:1419–31.
Article11. Brown DM, Kaiser PK, Michels M, et al. Ranibizumab versus verteporfin for neovascular age-related macular degeneration. N Engl J Med. 2006; 355:1432–44.
Article12. Lewis H. Intraoperative fibrinolysis of submacular hemorrhage with tissue plasminogen activator and surgical drainage. Am J Ophthalmol. 1994; 118:559–68.
Article13. Lim JI, Drews-Botsch C, Sternberg P Jr, et al. Submacular hemorrhage removal. Ophthalmology. 1995; 102:1393–9.
Article14. Ibanez HE, Williams DF, Thomas MA, et al. Surgical management of submacular hemorrhage. A series of 47 consecutive cases. Arch Ophthalmol. 1995; 113:62–9.15. Hassan AS, Johnson MW, Schneiderman TE, et al. Management of submacular hemorrhage with intravitreous tissue plasminogen activator injection and pneumatic displacement. Ophthalmology. 1999; 106:1900–6. discussion 1906–7.16. Lincoff H, Kreissig I. Intravitreal injection of tissue plasminogen activator and gas in subretinal hemorrhage caused by age-related macular degeneration. Retina. 2001; 21:191.
Article17. Cleary CA, Jungkim S, Ravikumar K, et al. Intravitreal bevacizumab in the treatment of neovascular age-related macular degeneration, 6- and 9-month results. Eye. 2008; 22:82–6.
Article18. Stifter E, Michels S, Prager F, et al. Intravitreal bevacizumab therapy for neovascular age-related macular degeneration with large submacular hemorrhage. Am J Ophthalmol. 2007; 144:886–92.
Article19. Fung AE, Lalwani GA, Rosenfeld PJ, et al. An optical coherence tomography-guided, variable dosing regimen with intravitreal ranibizumab (Lucentis) for neovascular age-related macular degeneration. Am J Ophthalmol. 2007; 143:566–83.
Article20. Brown MM, Brown GC, Sharma S, et al. The burden of age-related macular degeneration: a value-based analysis. Curr Opin Ophthalmol. 2006; 17:257–66.21. Schouten JS, La Heij EC, Webers CA, et al. A systematic review on the effect of bevacizumab in exudative age-related macular degeneration. Graefes Arch Clin Exp Ophthalmol. 2009; 247:1–11.
Article22. Kliffen M, Sharma HS, Mooy CM, Kerkvliet S. Increased expression of angiogenic growth factors in age-related maculopathy. Br J Ophthalmol. 1997; 81:154–62.
Article23. Rosenfeld PJ, Rich RM, Lalwani GA. Ranibizumab: Phase III clinical trial results. Ophthalmol Clin North Am. 2006; 19:361–72.24. Sacu S, Stifter E, Vécsei-Marlovits PV, et al. Management of extensive subfoveal haemorrhage secondary to neovascular age-related macular degeneration. Eye. 2009; 23:1404–10.
Article25. Meyer CH, Scholl HP, Eter N, et al. Combined treatment of acute subretinal haemorrhages with intravitreal recombined tissue plasminogen activator, expansile gas and bevacizumab: a retrospective pilot study. Acta Ophthalmol. 2008; 86:490–4.
Article26. Scupola A, Coscas G, Soubrane G, Balestrazzi E. Natural history of macular subretinal hemorrhage in age-related macular degeneration. Ophthalmologica. 1999; 213:97–102.
Article27. Bressler NM, Bressler SB, Childs AL, et al. Surgery for hemorrhagic choroidal neovascular lesions of age-related macular degeneration: ophthalmic findings: SST report no. 13. Ophthalmology. 2004; 111:1993–2006.28. Arias L, Monés J. Transconjunctival sutureless vitrectomy with tissue plasminogen activator, gas and intravitreal bevacizumab in the management of predominantly hemorrhagic age-related macular degeneration. Clin Ophthalmol. 2010; 4:67–72.
Article29. Rosa RH Jr, Davis JL, Eifrig CW. Clinicopathologic reports, case reports, and small case series: clinicopathologic correlation of idiopathic polypoidal choroidal vasculopathy. Arch Ophthalmol. 2002; 120:502–8.30. Tong JP, Chan WM, Liu DT, et al. Aqueous humor levels of vascular endothelial growth factor and pigment epithelium-derived factor in polypoidal choroidal vasculopathy and choroidal neovascularization. Am J Ophthalmol. 2006; 141:456–62.
Article31. Matsuoka M, Ogata N, Otsuji T, et al. Expression of pigment epithelium derived factor and vascular endothelial growth factor in choroidal neovascular membranes and polypoidal choroidal vasculopathy. Br J Ophthalmol. 2004; 88:809–15.
Article32. Hikichi T, Ohtsuka H, Higuchi M, et al. Improvement of angiographic findings of polypoidal choroidal vasculopathy after intravitreal injection of ranibizumab monthly for 3 months. Am J Ophthalmol. 2010; 150:674–82.
Article33. Uyama M, Wada M, Nagai Y, et al. Polypoidal choroidal vasculopathy: natural history. Am J Ophthalmol. 2002; 133:639–48.
- Full Text Links
-
- Actions
-
Cited
- CITED
-
- Close
- Share
-
- Similar articles
-
- Intravitreal Ranibizumab Therapy for Neovascular Age-Related Macular Degeneration with a Predominantly Hemorrhagic Lesion
- Intravitreal Aflibercept for Neovascular Age-Related Macular Degeneration Resistant to Bevacizumab and Ranibizumab
- Treatment of Exudative Age-Related Macular Degeneration
- Efficacy of Three Aflibercept Injections for Neovascular Age-related Macular Degeneration Showing Limited Response to Ranibizumab
- Comparison between Aflibercept, Ranibizumab Intravitreal Injection on Neovascular Age-related Macular Degeneration Patients
