A Promising Treatment for Broncholith Removal Using Cryotherapy during Flexible Bronchosopy: Two Case Reports
- Affiliations
-
- 1Division of Pulmonology, Critical Care Medicine, Department of Internal Medicine, Incheon St. Mary's Hospital, The Catholic University of Korea College of Medicine, Incheon, Korea. kimjusang@catholic.ac.kr
- KMID: 2050682
- DOI: http://doi.org/10.4046/trd.2012.73.5.282
Abstract
- Broncholiths are defined as calcified materials that occur in a tracheobronchial tree or in a cavity communicating with that. Broncholith has variable clinical features. The therapeutic options to remove broncholiths are so variable that clinicians need to select the most safe and effective methods by mass size, mobility, and location. As yet, there is no consistent guideline removing a broncholith. We report 2 successful cases of removing a fixed broncholith by flexible bronchoscopy guided cryoadhesion. With repeated technique of thawing and freezing with ryoprobe, we could extract the fixed broncholith safely. This method is promising as a way to remove broncholith in the future.
Keyword
Figure
-
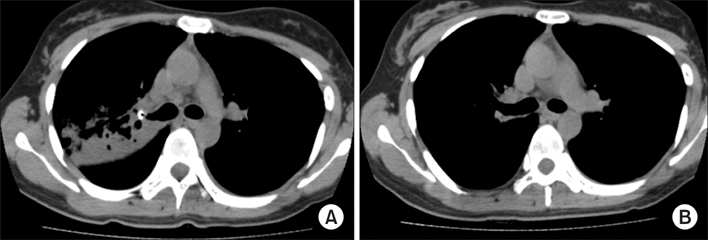
Figure 1 A 32-year-old woman's computed tomography (CT) scan image. (A) Chest CT scan image (mediastinal setting) showing calcifications present within the right upper lobe bronchus and resulting pneumonia. (B) Follow-up CT scan image (mediastinal setting) after bronchoscopic broncholith removal showing a patent airway and recovered pneumonic infiltrations.
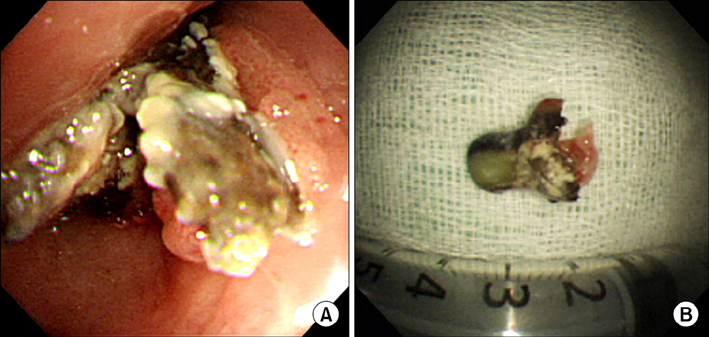
Figure 2 A 32-year-old woman's bronchoscopy image and extracted broncholiths. (A) The bronchoscopic view showing the sharp marginated broncholith which attached at the opening of the right upper lobe bronchus. (B) The extracted broncholith which was about 1.8 cm sized.
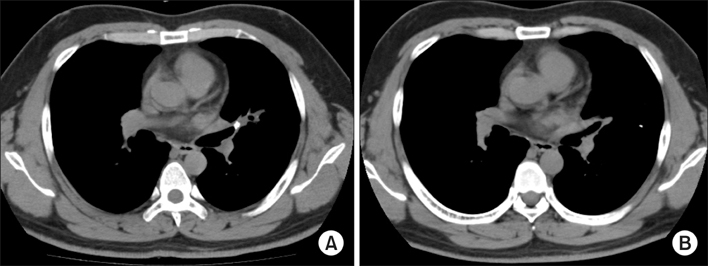
Figure 3 A 32-year-old man's computed tomography (CT) scan image. (A) Chest CT scan image (mediastinal setting) showing patchy opacities surrounding lingular segment and a calcified density within left upper lobe bronchus suggesting broncholith with pulmonary hemorrhage. (B) Follow-up CT scan image (mediastinal setting) after bronchoscopic broncholith removal showing no endobronchial mass.

Figure 4 A 32-year-old man's bronchoscopy image and extracted broncholiths. (A) The bronchoscopic view showing the impacted broncholith in the left upper lobe lingular division orifice. (B) The extracted broncholith was about 1.6 cm sized tooth-like yellowish mass.
Cited by 1 articles
-
Efficacy of Foreign Body Removal using a Cryoprobe in Flexible Bronchoscopy
Go Eun Yeo, Sung-Jin Nam, Yu Jin Han, Eun Jeong Kim, Nam Kyu Kim, So Young Ock, Weon Hyoung Lee, Chul Ho Oak, Mann Hong Jung, Tae Won Jang
Kosin Med J. 2014;29(1):31-36. doi: 10.7180/kmj.2014.29.1.31.
Reference
-
1. Kwak SM, Ahn CM, Kim HJ, Lee JS, Oh SH. A case of middle lobe syndrome due to broncholithiasis. Korean J Intern Med. 1988. 34:834–840.2. Lee HL, Kim SK, Chang J, Kim SK, Lee WY, Chung KY. A study on broncholithiasis. Korean J Med. 1995. 48:353–361.3. Yi KY, Lee HK, Park SJ, Lee YC, Rhee YK, Lee HB. Two cases of broncholith removal under the guidance of flexible bronchoscopy. Korean J Intern Med. 2005. 20:90–91.4. Olson EJ, Utz JP, Prakash UB. Therapeutic bronchoscopy in broncholithiasis. Am J Respir Crit Care Med. 1999. 160:766–770.5. Ferguson JS, Rippentrop JM, Fallon B, Ross AF, McLennan G. Management of obstructing pulmonary broncholithiasis with three-dimensional imaging and holmium laser lithotripsy. Chest. 2006. 130:909–912.6. Cerfolio RJ, Bryant AS, Maniscalco L. Rigid bronchoscopy and surgical resection for broncholithiasis and calcified mediastinal lymph nodes. J Thorac Cardiovasc Surg. 2008. 136:186–190.7. Miks VM, Kvale PA, Riddle JM, Lewis JW Jr. Broncholith removal using the YAG laser. Chest. 1986. 90:295–297.8. Bolliger CT, Mathur PN, Beamis JF, Becker HD, Cavaliere S, Colt H, et al. ERS/ATS statement on interventional pulmonology. European Respiratory Society/American Thoracic Society. Eur Respir J. 2002. 19:356–373.9. Ernst A, Feller-Kopman D, Becker HD, Mehta AC. Central airway obstruction. Am J Respir Crit Care Med. 2004. 169:1278–1297.10. Asimakopoulos G, Beeson J, Evans J, Maiwand MO. Cryosurgery for malignant endobronchial tumors: analysis of outcome. Chest. 2005. 127:2007–2014.11. Reddy AJ, Govert JA, Sporn TA, Wahidi MM. Broncholith removal using cryotherapy during flexible bronchoscopy: a case report. Chest. 2007. 132:1661–1663.12. Tellides G, Ugurlu BS, Kim RW, Hammond GL. Pathogenesis of systemic air embolism during bronchoscopic Nd:YAG laser operations. Ann Thorac Surg. 1998. 65:930–934.13. Kim HO, Kim SJ, Lee SH, Lee EJ, Hur GY, Lee SY, et al. A case of atypical bronchial carcinoid treated by cryotherapy. Tuberc Respir Dis. 2011. 70:521–525.14. Lyu J, Song JW, Hong SB, Oh YM, Shim TS, Lim CM, et al. Bronchoscopic cryotherapy in patients with central airway obstruction. Tuberc Respir Dis. 2010. 68:6–9.15. Jung JY, Lee SY, Kim DH, Lee KJ, Lee EJ, Kang EH, et al. Clinical benefits and complications of cryotherapy in advanced lung cancer with central airway obstruction. Tuberc Respir Dis. 2008. 64:272–277.
- Full Text Links
-
- Actions
-
Cited
- CITED
-
- Close
- Share
-
- Similar articles
-
- A Promising Treatment for Broncholith Removal Using Cryotherapy during Flexible Bronchosopy: Two Case Reports
- A Case of Endobronchial Actinomycosis with a Broncholith cured by Cryotherapy through a Flexible Bronchoscope
- Two Cases of Broncholith Removal under the Guidance of Flexible Bronchoscopy
- A Case of Broncholithiasis, which was Treated by Flexible Bronchofiberscopy
- Broncholithiasis Caused by Actinomycosis
