A Case of Pulmonary Paragonimiasis Presented as Solitary Pulmonary Nodule and Suspected as Lung Cancer on (18)F-Fluorodeoxyglucose Positron Emission Tomography
- Affiliations
-
- 1Department of Internal Medicine, Ansan Hospital, Korea University College of Medicine, Ansan, Korea. chepraxis@korea.ac.kr
- 2Department of Thoracic and Cardiovascular Surgery, Ansan Hospital, Korea University College of Medicine, Ansan, Korea.
- 3Department of Pathology, Ansan Hospital, Korea University College of Medicine, Ansan, Korea.
Abstract
- Pulmonary paragonimiasis continues to be a diagnostically challenging parasitic disease, despite a drastically decreased prevalence in South Korea during the past decade. Pulmonary paragonimiasis is characterized by fever, chest pain, and chronic cough with hemoptysis. Numerous radiographic and computed tomographic findings including the presence of pneumothorax, pleural effusion, and parenchymal lesions such as nodular or infiltrative opacities have been reported. The clinical and radiological manifestations of paragonimiasis can resemble those of lung cancer, tuberculosis or a metastatic malignancy. Furthermore, this disease can mimic lung cancer as seen on 18F-fluorodeoxyglucose positron emission tomography (FDG-PET). We report a case of pulmonary paragonimiasis in a 48-year old man that presented with a solitary pulmonary nodule and was suspected as a lung cancer based on FDG-PET imaging.
MeSH Terms
Figure
-
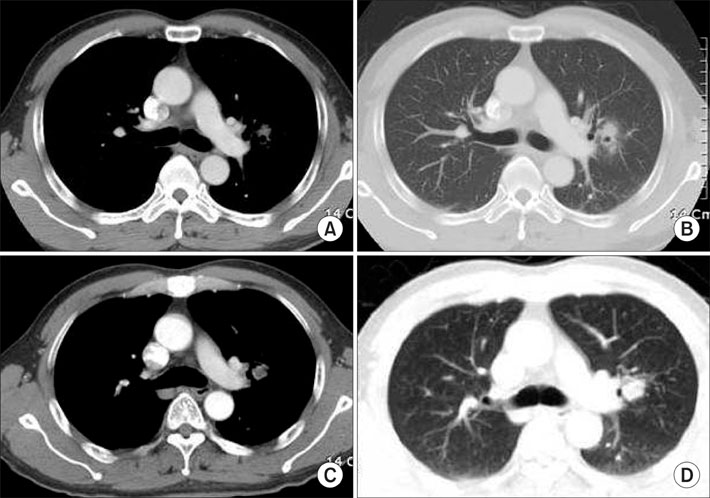
Figure 1 Chest computed tomography (CT) showed ill-defined nodular consolidation at apicoposterior segment of left upper lobe (A, B). The size of this spiculate lesion enlarged with increase of solid component, 2 months later (C, D).

Figure 2 There was about 2×2.5 cm sized hypermetabolized lung nodule with peripheral ground glass opacity (GGO) in hilar area of left upper lobe (pSUV 3.9 g/ml). Mild increased FDG uptake in left hilar node, suggestive of lymph node metastasis, was also noted.
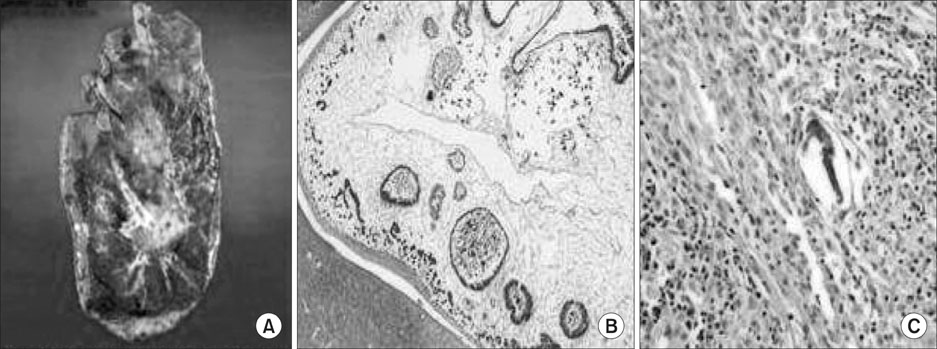
Figure 3 Gross specimen of left upper lobe (A) showed a poorly demarcated multilocular yellowish gray cystic lesion at the cut surface, measuring 2×2.4 cm. Histology of the resected mass revealed chronic granulomatous inflammation with adult parasite and many eggs, consistent with paragonimiasis (B, C. hematoxylin and eosin, ×200, ×400).
Reference
-
1. Kuzucu A. Parasitic diseases of the respiratory tract. Curr Opin Pulm Med. 2006. 12:212–221.2. Nawa Y. Re-emergence of paragonimiasis. Intern Med. 2000. 39:353–354.3. Im JG, Whang HY, Kim WS, Han MC, Shim YS, Cho SY. Pleuropulmonary paragonimiasis: radiologic findings in 71 patients. AJR Am J Roentgenol. 1992. 159:39–43.4. Croft DR, Trapp J, Kernstine K, Kirchner P, Mullan B, Galvin J, et al. FDG-PET imaging and the diagnosis of non-small cell lung cancer in a region of high histoplasmosis prevalence. Lung Cancer. 2002. 36:297–301.5. Yu YK, Kim KS, Kim YH, Nah KJ, Kim KS, Lim SC, et al. A case of the solitary pulmonary nodule diagnosed as pulmonary paragonimiasis. Chonnam Med J. 2001. 37:185–188.6. Cho SY, Kong Y, Kang SY. Epidemiology of paragonimiasis in Korea. Southeast Asian J Trop Med Public Health. 1997. 28 Suppl 1:32–36.7. Nakamura-Uchiyama F, Mukae H, Nawa Y. Paragonimiasis: a Japanese perspective. Clin Chest Med. 2002. 23:409–420.8. Jeon K, Koh WJ, Kim H, Kwon OJ, Kim TS, Lee KS, et al. Clinical features of recently diagnosed pulmonary paragonimiasis in Korea. Chest. 2005. 128:1423–1430.9. Lee CH, Im JG, Goo JM, Lee HJ, Hong ST, Shen CH, et al. Serial CT findings of Paragonimus infested dogs and the Micro-CT findings of the worm cysts. Korean J Radiol. 2007. 8:372–381.10. Tomita M, Matsuzaki Y, Nawa Y, Onitsuka T. Pulmonary paragonimiasis referred to the department of surgery. Ann Thorac Cardiovasc Surg. 2000. 6:295–298.11. Kim TS, Han J, Shim SS, Jeon K, Koh WJ, Lee I, et al. Pleuropulmonary paragonimiasis: CT findings in 31 patients. AJR Am J Roentgenol. 2005. 185:616–621.12. Detterbeck FC, Falen S, Rivera MP, Halle JS, Socinski MA. Seeking a home for a PET, part 1: defining the appropriate place for positron emission tomography imaging in the diagnosis of pulmonary nodules or masses. Chest. 2004. 125:2294–2299.13. Goo JM, Im JG, Do KH, Yeo JS, Seo JB, Kim HY, et al. Pulmonary tuberculoma evaluated by means of FDG PET: findings in 10 cases. Radiology. 2000. 216:117–121.14. Reuter S, Schirrmeister H, Kratzer W, Dreweck C, Reske SN, Kern P. Pericystic metabolic activity in alveolar echinococcosis: assessment and follow-up by positron emission tomography. Clin Infect Dis. 1999. 29:1157–1163.15. Yoo IeR, Park HJ, Hyun J, Chung YA, Sohn HS, Chung SK, et al. Two cases of pulmonary paragonimiasis on FDG-PET CT imaging. Ann Nucl Med. 2006. 20:311–315.
- Full Text Links
-
- Actions
-
Cited
- CITED
-
- Close
- Share
-
- Similar articles
-
- A Case of Pulmonary Paragonimiasis Presented as Solitary Pulmonary Nodule and Suspected as Lung Cancer on (18)F-Fluorodeoxyglucose Positron Emission Tomography
- A Pulmonary Paragonimiasis Case Mimicking Metastatic Pulmonary Tumor
- Computer-Aided Differential Diagnosis of the Pulmonary Nodule: Towards an Understanding of the Medical Imaging Basics and Experiences in the Field
- A Case of the Solitary Pulmonary Nodule Diagnosed as Pulmonary Paragonimiasis
- Bronchioloalveolar Cell Carcinoma in Solitary Pulmonary Nodule(SPN) with Cavitary Lesion
